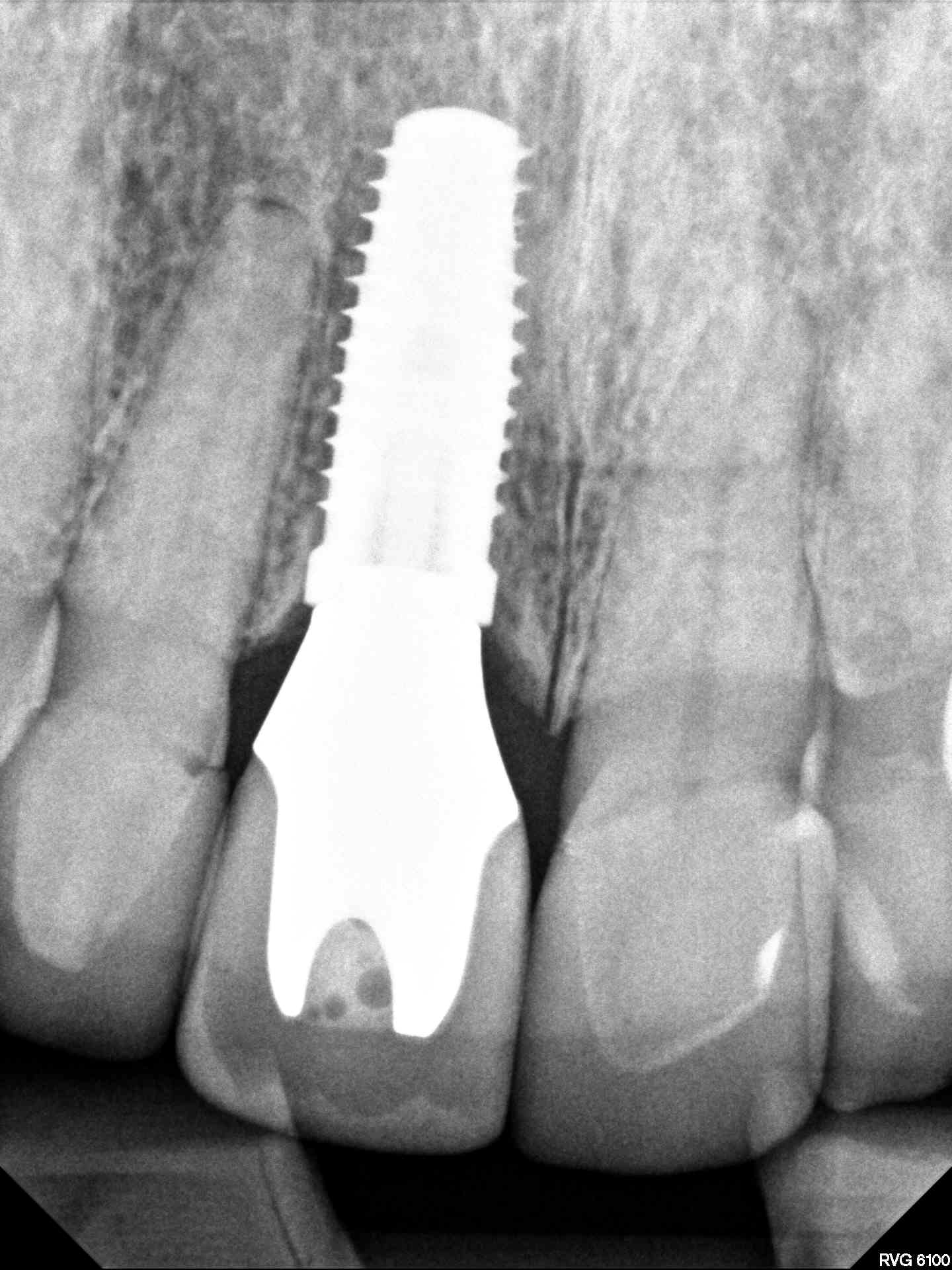
This patient was referred to me because the referring doc could not remove the stripped abutment screw on #14. Apparently #3 and #14 are Neodent fixtures and I am wondering WHY??? Could somebody please justify this concept of small platform fixtures placed subcrestal. I am sorry but this concept makes absolutely no sense and I am hoping that somebody on this forum can shed some light as to why anyone would think this is a good idea when restoring a posterior tooth…

I completely understand the concept of medialized abutments, platform switching, etc… That is not what this concept is. When it comes to restoring posterior teeth size does matter and when molar contours are being attempted from a 1-2mm subcrestal implant platform of 3mm problems are iminent. This is a ridiculous deviation from common sense.
So,
Just for clarification, your issue is 1) 2mm Sub-crestal placement of Regular width vs Narrow width Implants Vs. (2) Narrow implants placed sub-crestally in Posterior segments? Vs. (3) Since prosthetic jxn of Neodent is the same all across, and Narrow, Neodent implants should Not be used for Posterior segments.
I agree with you, You need at least a 4.3mm implant when going posterior of Pre-molar regions. However Platform issue is more geard for Restorative doctors, very simple and easy for most practitioners, new or older practitioners.
The records indicate that it is a 4.3 Neodent and the ridiculousness of the concept is visible. This system thinks it ok to have a standard/universal connection all in the name of simplicity. Just take a look at the image and it is clear that this is a flawed concept. The fact that the platform is so small requires a subcrestal placement which further compromises, if you consider it important, the implant:crown. Just because something is easy doesn’t make it right and I have no doubt that history will dispose of this concept in the same manner that it has unintentionally proven the superiority of the opposite concept, which is wide platform tissue level fixtures for the replacement of posterior teeth.
I hear you about everything being one size and it being a big issue with regards to complications such as this; and using wider collars in posterior implants makes more sense. That said, I place Neodent or Nobel and they both have their Pluses and Minuses.
Neodent has a screw retrieval kit which you can get from them to make your life easier.
I don’t understand what is ridiculous about subcrestal placement and platform switching?
The implant needs to be wide enough so that it doesn’t fracture. Subcrestal placement with a conical connection and platform switch all contribute to crestal bone stability. I don’t place Neodent so I can’t comment on 4.3mm diameter for a Molar. Subcrestal placement of 2mm plus 3mm (guess) tissue height give 5mm of running room to develop the proper emergence. Subcrestal placement is problematic for internal hex implants but not so for connical connection implants. Neodent has a 16 degree morse taper so should be fine for subcrestal placement.
If you don’t mind me asking… “Why Neodent”? I am a loyal Zimmer guy who has experience with Nobel, 3i, Straumann, Bio Horizon, Zimmer, and Blue Sky Bio but landed on Zimmer about 10 years ago as my go to product. My only issue with Zimmer is that they do not have a wide platform tissue level fixture so I resort back to the trusty Blue Sky Bio One Stage for this. I am currently in the process of designing a new product with ZimVie (formerly Zimmer) to address this issue and eliminate the need for me to utilize another system. Neodent just seems like a another cheap product designed for the discount minded doctor hiding behind the veil of Straumann Group. I had a Neodent rep stop by my office about 3-4 weeks ago and offer me all sorts of free stuff just to try their product. I politely said no and when she wouldn’t give up I simply showed her this picture and asked her “why” would I do this to my patients… she left my office and she hasn’t bothered me since.
At least the short term data would support your claim but short term data also propelled the Nobel Tri Lobe to number one in the world before history told the truth on this . Despite our attempts to rewrite history and create easier to use products the data suggests a different concept for the long term restoration of posterior teeth.
Why would you ever need 5mm of running room to restore a posterior tooth??? Unless you were attempting to emerge from an insufficient platform?
Neodent is owned by Straumann and we don’t usually hear people complain that Straumann is a low cost implant company. I don’t place Neodent and only some Straumann so I’m not pushing their case. I’m simply stating that subcrestal placement of a conical connection implant with platform switch is well documented recipe for crestal bone stability in the literature.
“Why would you ever need 5mm of running room to restore a posterior tooth?” Vertical tissue height between the free gingival margin and the implant platform is a known factor for crestal bone stability.
When we platform swich (another proven method to achieve crestal bone stability) then we by definition switch to a smaller diameter even if we have a 6mm diameter implant. Then the implant needs to be placed deeper subcrestally in order to achieve the proper emergence. Your reference to insufficient platform may be your personal preference but its not evidence based fact.
1 Like
Straumann is not a discount product and Neodent is not Straumann… but it is owned by Straumann Group and that veil of quality earns it some unnecessary traction. 3i invented the concept of platform switching and I am quite familiar but at no time were we ever encouraged to platform switch/emerge a posterior tooth from a 3mm platform. Maybe a 4mm emergence from a 5mm fixture or 5mm from a 6mm diameter but never from 3mm. After 20 years as a practicing periodontist I have still never seen a posterior tooth that needs 5 mm of running room and I have seen a lot of thick gingiva, in fact I have augmented to establish a lot of thick gingiva and this is just not reality.
No one spoke of a 3mm platform. Your example is a 4.3mm platform.
Look up Zero Bone Loss Concepts and you will see endless periapicals with bone all over the implant platform and 5+mm between the free gingival margin and the implant platform for molars. I’m guessing that if you look back at periapicals of your internal hex implants placed at the crest or supra, you will see crestal bone loss in most of the cases.
Bottom line is that this product, Neodent, is leaning on the concept of universal platform for simplicity with no regard for common sense. If simple always won then we would all still be placing and restoring Nobel Tri Lobe because it is incredibly simple… it just doesn’t do well long term. Platform switching has been around a long time and is well documented but this subcrestal placement of tiny platform conical fixtures is just lipstick on a pig. Attached is a 10 years follow up on a platform switched 3i fixture (5mm fixture restored with 4mm prosthetics).
The platform/connection on this 4.3mm fixture is a 3mm universal restorative platform, which is too small to establish proper contours for a posterior tooth. There may be 5+mm of running room with no evidence of bone loss on the periapicals you speak of but it still doesn’t pass the sniff test. I have literally thousands of fixtures placed crestally with evidence of crestal bone loss which is precisely why I reverted back to tissue level fixtures for the restoration of posterior teeth. These fixtures have no bone loss and they have a reasonable emergence profile. Platform size matters with posterior teeth and this concept ignores this reality… but it is simple for the doc…
“I have literally thousands of fixtures placed crestally with evidence of crestal bone loss.”
Why are you bragging about having thousands of implants with crestal bone loss?
Sometimes a little bone loss progresses to failure.
I prefer to avoid bone loss on my implants.
Thats why I practice Zero Bone Loss Concepts and place conical connection implants subcrestally, many times 5+ mm below the free gingival margin with bone predictably up to the top of the implant platform. The “sniff test” is not evidence based and just your personal opinion.
1 Like
I am not bragging I am admitting the error of my ways. I realized there was a problem with crestally placed bone level fixtures and I went back to the basics of tissue level to solve this issue. The tissue level concept has over 30 years of evidence but it will never dominate because it is slightly more difficult to place these tissue level fixtures. I agree with the idea but placing a tiny platform way subcrestal is something that I honestly believe history will take care of the same way it supports the opposite or tissue level concept.
The next time you find yourself needing to remove one of these restorations built on a 5mm subgingival 2mm subcrestal fixture I would encourage you to inhale deeply and then see if you agree with the sniff test. To the best of my knowledge there is no predictable soft tissue attachment to an implant and the bugs that can reside in this space don’t have the most pleasant smell so in this case the sniff test is much more than just an opinion.
Why Neodent? Let me start with, I DON’T have any relation or investment in Neodent, and not endorsing the product for sale here. I use Neodent because it’s a Good product, especially about lowering the stress points deep into the fixture for better bone support. Engineering wise makes sense. Also, doing that helps you get more running room for soft tissue, whereby if the Hemidesmosome seal has formed chances of bacterial invasion are low. The Morse taper forms a tight seal, almost cold weld with the implant internals.
If you think Neodent is a “Cheap product for discount minded doctor”, well then I guess you pooh pooh everyone who places MIS, or ADIN or the next dujour implant company selling implants for $50, so that is your own assumption/perspective, because Neodent is NOT the cheapest implant out there. Price plays some role but not everything. From your contention, Osteoblasts know when you placed a Straumann vs. Neodent implant? Because both have same SLA coating, but cells can tell.
Now, you can debate any implant systems pros and cons, however we are constantly working with newer knowledge in order to get better overall results for our patients, that being the motivating factor for most of us clinicians. For example I really like the new Nobel product with Oval connical N1, seems to make a lot of sense NOT to Crush the bone at the Crest of the osteotomy and allow for blood to seal with a soft seal. How well it works will bear out over time.
My $0.02
If it works for you and makes sense then keep it up… Does it actually make sense to emerge a molar from a 3mm universal platform though. I can go on all day about the pros and cons of every system but the data always takes me back to the tried and true tissue level concept that I foolishly abandoned based on market trends years ago. Now seeing my own patients come back with 10-15 year old fixtures I can do more than rely on silver tongue sales reps and flashy CE courses and utilize my own success and failure to dictate my plans. Conical is good, platform switching is good, medialized abutments are good, tissue level is good… they all work but this concept for posterior teeth is flawed and I have no doubt that history will confirm this. And by the way while I often reference Straumann it is Blue Sky Bio One Stage that I resort to because it works and it has the added benefit of being inexpensive as well.
The problem with tissue level fixtures is that there is a textured part and a polished part, and the idea is to place the textured part in the bone and the polished part in the tissue. This assumes a perfectly flat level alveolar crest. This is not the reality of the alveolar crest. The ridge is typically more the shape of a pringles potato or a horse saddle. Then when you place it, the transition line will be partially supracrestal and part subcrestal. Having the polished part subcrestal will result in bone loss 100% of the time. Having the textured part supracrestal is not great either. You could plasty the ridge flat, but why drill away good bone when you can just place a conical implant subcrestal?
MIS has a transmucosal abutment called the Connect abutment in different tissue heights, and it transforms the V3 implant into closer to tissue level platform.
I’m not suggesting a tiny platform for molar implants. I’m suggesting that there is more than one way to skin a cat. When your tissue level implant gets a mm or two of recession then the metal is exposed and that’s not easy to fix. If you used a Connect abutment, you could always remove the Connect abutment and place a shorter one.
There are multiple papers that show highly polished Zirconia has a favorable response in peri-implant tissues, with lower plaque adhesion, lower tissue inflammation and better esthetics. Hemidesmosomal attachment is better with Zirconia than titanium. So, when we place a conical implant deeper subcrestal we can have more tissue Zirconia interface which makes a seal and contributes to crestal bone stability.