I hear you about 3mm wide platform, and emerging from that, especially in Posterior segments however I haven’t had issues with needing to retrieve a screw from posterior areas, yet. If and When it happens, I am sure I will be muttering under my breath. I did have a 91 yrs old patient break abut screws of an straight Multi-unit abut in anterior Maxilla, and trying to retrieve that screw was Impossible, had to explant and go with another implant.
Tissue levels are not Panacea because of Patient’s tongues, and other habits such as ice chewing etc. that mess with anything above bone and lead to issues with Osteointegration, and early bone loss. I have had patients almost cause loss of crestal bone due to playing with healing abut on a Nobel Active 3.5 in #28 site and other implants with Supra-crestal healing abuts.
So, I am not necessarily saying that a wider implant internal aspect is NOT better, because making a custom abut, which I use most of the time, is easier with wider platform. However we need to understand that the wider connection is coming at cost of thickness of Titanium at the Neck of the implant and crestal level, and that could “FLOWER” too.
So, there is no 100% fool proof option. Patient selection should/could dictate implant type selection, for e.g. bruxers, need implants burried, at least for osseointegration phase.
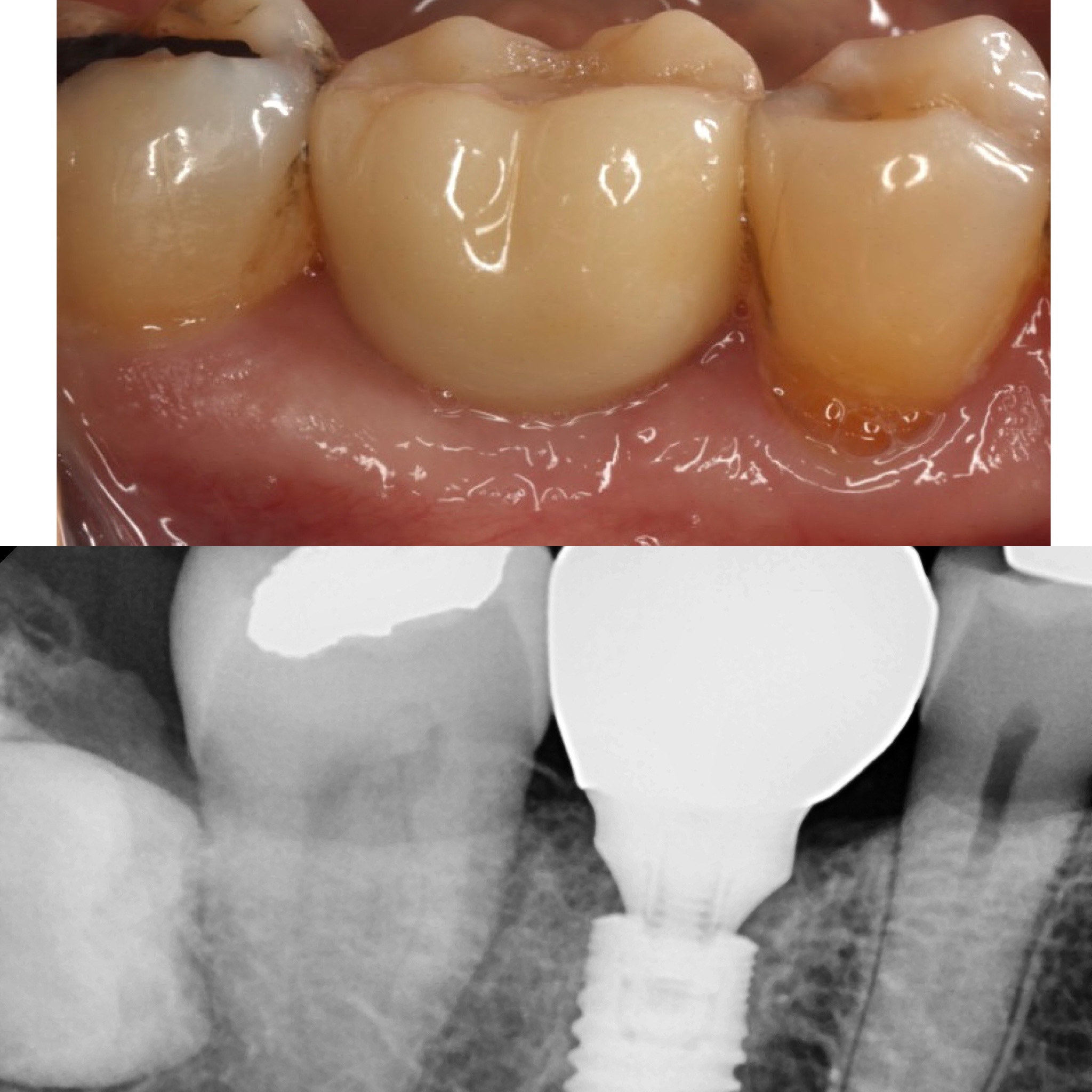
Looking at pano, #14 implant does look thin. There is plenty of space mesial/distal of implant for a wider implant. But how about CBCT? Although on PA/PANO mesial/distally looks lots of space for a >5mm implant. Very often buccal/lingually long time edentulous sites resorbs. your limited to use a smaller implant to accommodate thing buccal/lingual alveolar ridge dimensions. I wouldn’t fault surgeon using a thinner implant just because you think should be thicker. We all want to overengineer and place as large as an implant as possible, pending alveolar ridge dimensions. I would have also do sinus lift to place >10mm long implants as well. But honestly how many of us try to save patient money and comorbidities by avoiding sinus lifts and placing a shorter implants? Upper implants suffer more translational forces thus longer upper implants tend to have better prognosis. So before you reject a smaller implant for posterior, take a CBCT and eval the bone. perhaps the previous surgeon placed a smaller implant due to thin alveolar ridge and decided not to GBR to thicken the ridge before hand since treatment time would be prolonged and finances would increase for patient.
More importantly, were you able to remove the screw. Seems like the best part is that the abut is there, which can act as your guide to remove the Top of the screw. Then the abut should be able to shimmy out and you can use an Endo forcep or a Mosquito hemostat and twist the screw out. Just an idea, not sure if it will work.
Yes I did and I will just restore it with a new restoration. Another issue I have with this concept is that an area which could accept a 10mm long fixture will have to settle for an 8mm due to the subcrestal protocol. This concept also poses an issue for anyone electing to do a simultaneous implant placement and sinus lift. I remember years ago Fugazzotto speaking about proper fixture selection for anyone, like myself, electing to do implant at the time of sinus lift. We were encouraged to use a fixture with a flared healing abutment or better yet a tissue level fixture, Fugazzotto is a Straumann disciple, to guard against the possibility of the fixture being displaced into the sinus. I have personally done the vast majority of my simultaneous implant/sinus lift procedures utilizing a Zimmer TSV with a flared healing abutment at the time of placement or with a Blue Sky Bio One Stage. I rarely, unless there is a removable appliance involved, submerge any implant fixture as I am a firm believer that it is just not necessary and I really hate numbing a patient just to uncover a screw.
I think it is important to note that at no time was the surgeon that placed this being criticized. This discussion was initiated to discuss a concept which was used… and from what I have learned about this system which I do not like this particular surgeon did a good job of practicing the concept.
@dr-moe and @theimplantdoc thank you for a productive discussion as I have certainly been educated on a concept which I don’t fully comprehend or agree with. While the discussion may not inspire me to run out and buy a bunch of Neodent merchandise I can certainly appreciate certain situations where this concept might be beneficial. Thanks again and hopefully more discussions like this can transpire in the future.
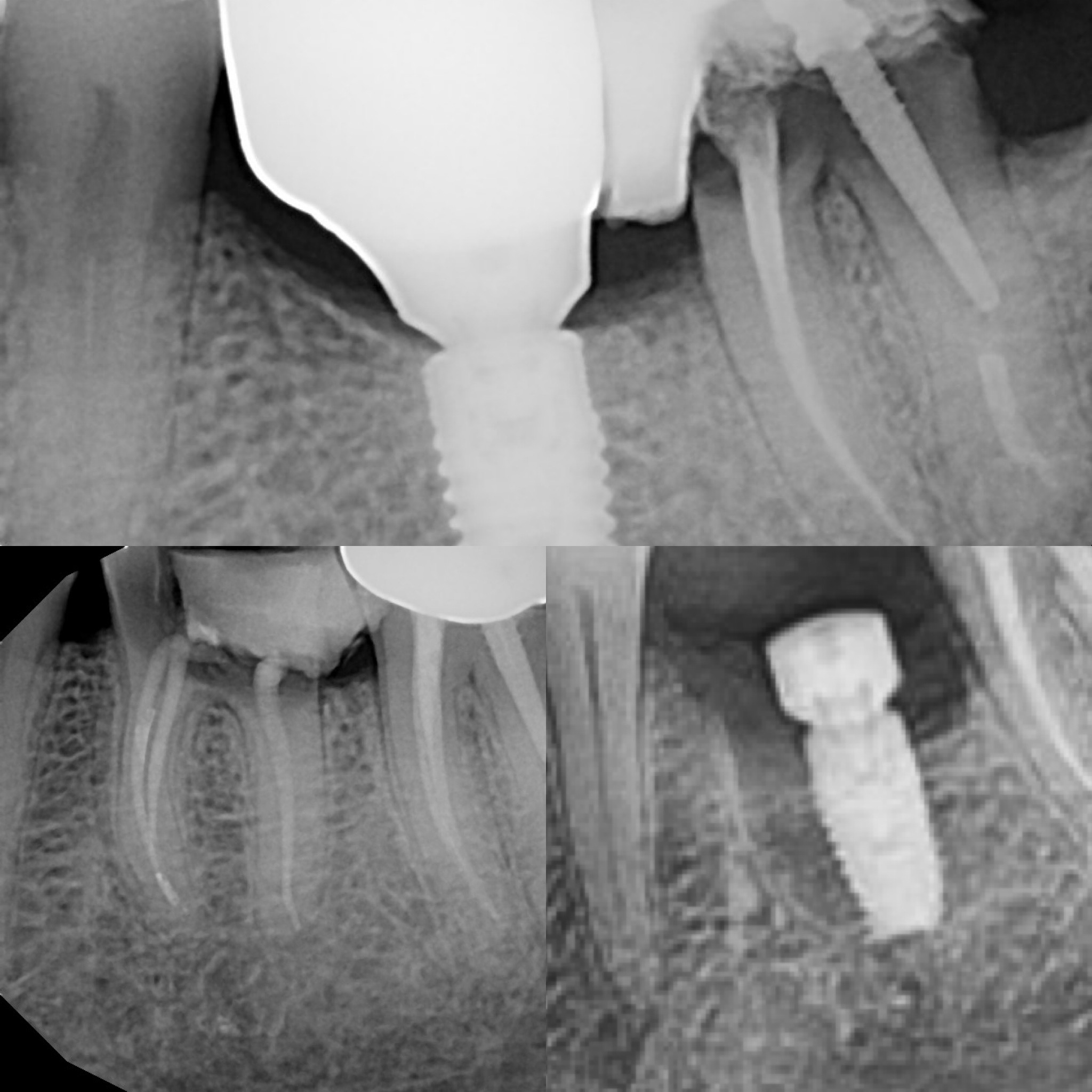
First time posting a photo here, don’t know if this will work. This is a four year follow up periapical of deeply placed MIS V3 with a Connect abutment. Bone all over the top of the implant.
This is great and for each one of these your prosthetic abutment is flared giving the restoration the proper seating surface for the tooth being restored. If you look at the case that I posted this is not the same. That individual used a fixture with a small conical connection and failed to attach a properly flared abutment. I think you might be understanding and properly utilizing this concept a little better than what I have seen from the staff at the local Affordable Denture facility in town…
@scotty,
Thanks for the discussion, every problem/complication is an opportunity to learn, once you are done washing your pants. =)
BTW,
The screw stripping part in Neodent could be due to Restorative doctor Torquing Neodent abutment screws too much. Neodent only recommends Torquing it’s Abut screws to 20Ncms, and I have found at times due to Morse taper, you just need to Hand tighten Neodent crowns and they don’t get loose. Because of the Morse taper, I have had problems with abuts getting cold welded, however in that case the Rep informed me to tap on the abut from bucco-lingual aspect and that does seem to loosen the abut. Just trying to figure out why this Screw was stripped.
I think it is most likely because Neodent has a proprietary star grip driver and the restorative doc likely tried to use a .048 or .050 standard hex driver. At any rate it was retrieved and the fixture will remain in place with a new restoration. That cold weld you speak of is important as that is what attracted me to Zimmer 10 years ago. Implant Direct will try and claim to be the same but if you place a genuine Zimmer abutment on a Zimmer implant then remove the screw the abutment will stay in place and may require a special abutment removal tool included in the surgery kit. If you do the same with Implant Direct the abutment will fall right off which is proof that Dr. Niznik did not retain the full patent. I think as long as we recognize these intricate details then we will all continue to use different but acceptable products for our patients. What drives me crazy is the folks that place a specific system, the Bio Horizons camp is the worst at this, simply because that is what they trained with and they don’t know any other product. One thing is for certain and that is that this is not a one size fits all practice…
so zimmer implants have a polished collar…is anyone saying you should not shoot for crestal or slightly subcrestal placement (like .5-1 mm subcrestal) or just crestal. Seems like I’ve had problems years ago when supracrestal.
Hi Scott,
Neodent and Nobel PMC CC has a 0.75mm polished collar, and Yes I place them approx. 1.0mm sub-osseous because Supra-crestal we have to worry about Patient habits which seems to lead to bone loss crestally due to tongue, ice chewing and other issues.
Also, I have noted that doing it that way you get some running room for the soft tissue.
Another issue is when thick cortical bone is present in the site where you are placing the implant. If the bone collar by the top of the implant is 2mm thick cortical bone, and you don’t create space between the collar and the bone, ie. profile it, you will get “bone loss” as it remodels, hence placing it sub-crestal works then too.
Just my 0.02 cents
I would never suggest to routinely place any bone level fixture supracrestal and subcrestal placement has been a proven method to facilitate running room/emergence for many years. The issue I have is the concept of using a small, usually 3.5mm, universal platform on fixtures routinely placed, per manufacturer, 1-2mm subcrestal for no other reason thea to show off the concept of the medialialized abutment. Conical connection is fine but it doesn’t have to be buried in order to be beneficial and effective. When a company like Neodent only makes one universal restorative platform I think they are contributing to the biggest problem in this field which is oversimplification. I honestly believe that there is a good reason that fixtures come in various sizes and standardizing a platform essentially takes us back to the old days of 3.75mm Branemark fixtures. One of you is likely going to try and correct this statement by saying that these products have multiple diameters and I agree but they have only one restorative platform to emergence from and that platform is the same for a lateral incisor as it is for a molar meaning unnecessary excessive subcrestal placement…