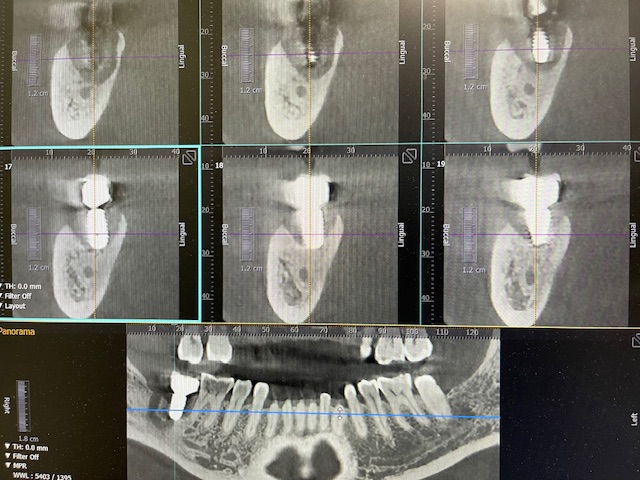
This #31 implant/crown was placed by a GP at one of the offices i work at. He placed in 2021 using a surgical guide. At 3 yr follow up which was 6 months ago, PA show bone around implant w/o any problems (ON THE RIGHT). but last week, a more current PA (ON THE LEFT) shows severe bone loss on the distal of the implant. only complaint by pt was bleeding at the implant and occasional discomfort and mild pain. CBCT taken.
I didn’t find any fault with #31 implant/crown. occlusion was good. crown size and position of implant was WNL.
I end up removing implant, PARL, and grafting the defect.
The only think i can think of is parafunction, but how did parafunction cause bone loss at 3 year post placement/restore and within a short period of 6 months, instead of immediately after restoration? I was very puzzled.
Any dr have some insight please? TIA.
After many years and many failures of my own I have come to the conclusion that sometimes this stuff just happens and there is nothing we could have, should have, or can do about it. One interesting thing I have found though is that this same thing tends to happen to mandibular second molar teeth as well where they just deteriorate quickly with no clear reason why other than it is a mandibular second molar. It is for reasons like this that I strongly discourage, some might accuse me of talking my patients out of replacing lower second molars. It is an area of the mouth that is difficult to treat, difficult to clean, and mathematically speaking second molars make up an insignificant portion of our chewing function and I have essentially retired from replacing them. Seriously though pay attention to how often mandibular second molar teeth just go downhill and then decide if the same thing might be expected for mandibular second molar screws…
I have also seen a few cases like this over the 20 years of placing and restoring. I believe part of the problem is many people have a hard time keeping the area behind second molars clean, and it is a prime spot for getting something stuck behind the distal of the implant. Other than that, can’t see why this would have occurred.
Could be bruxism. Occlusal guards are way under utilized. People are stressed these days. It’s one of the reasons those lower 2nd molars split and need extraction. One of the most stressed areas in the mouth.
For those of us that do implants , it’s only a matter of time until we see failures and as much as we want to avoid them, they are unfortunately part and parcel of doing them.It seems like it is part of the equation and one can only speculate why a case goes south on us and fails, especially when we do one by the book Sometimes there is no rhyme nor reason but it’s something that we and our patients have to live with. There is absolutely nothing wrong with ending the occlusion on the first molars or 2nd bicuspids and having the patient live with a shortend dental arch
Okay so I’m going to suggest a probable cause based on the radiographs you showed. There is a very light/to no contact on the mesial of the implant. Nothing creates peri-implantitis like food impaction. And the typical appearance is a cup shaped lesion that looks worse on the distal. Not likely parafunction, those look like a steep vertical defect or patient just reports all of a sudden pain and the last radiograph looked perfect.
I’m wondering if there had been infection in the past in this area and perhaps why tooth 31 was originally lost. I don’t know if it was an immediate implant… The shape of the bone loss suggests a possible cyst perhaps from microbes in the bone? I would’ve sent the distal bone defect contents out for pathological evaluation. I’ve never seen an implant fail with that shape of associated bone loss.
i didn’t place the 1st implant. so i didn’t investigate that much. I know it was done in 2 stages. 1st extraction and allograft placed. after 4-6 months a hiossen implant was placed.
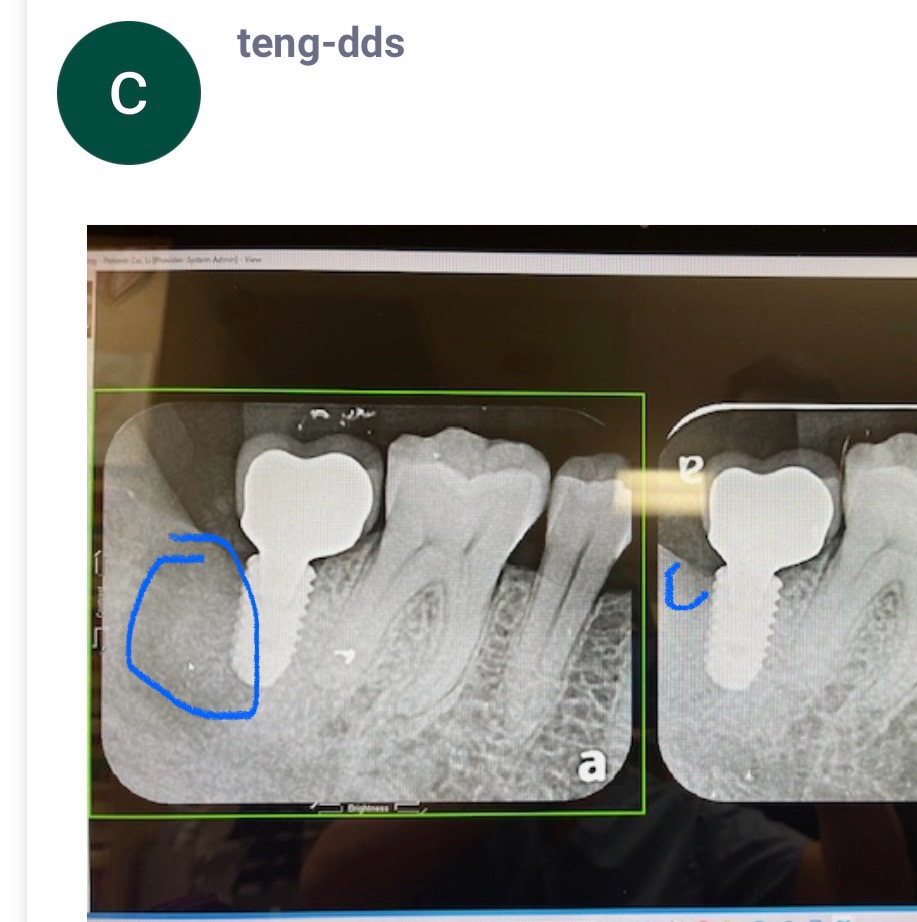
Please locate the X-ray from the time the infected tooth was extracted. It’s good practice to ask the question “Why did it fail” because that’s how we learn, but sometimes it takes some effort to gather the information. I’m guessing that the defect looked like my big blue circle. So the implant (internal hex connection) is in mostly graft on the distal. Combine this with the internal hex connection with only 2mm of tissue thickness on the distal and you can see the beginning of demineralization on the distal circles with the small blue line.
This is another example of why it’s better practice to place the implant immediately whenever possible because then you Know what the real insertion torque is in native bone. When you place your implant into a mass of graft, it might look nice radiograpgically, but it may not have the biomechanical ability to hold up to load.
Check out Ahmed Mataria’s course on the Prosthetic Considerations for Implant dentistry and you will learn how to accurately diagnose every failure.
Hello Buddy, for sure a food trap can lead to peri-implantitis and bone loss, but I think if there was a food trap on the mesial, the bone loss would have been on the mesial, however it was distal.
Occlusal forces will cause prosthetic failure not bone loss. The bone loss is because the biological width was not respected. We need at least 4mm of vertical tissue height between the free gingival margin and the platform of the implant. There was markedly less than that on the distal.
You can see it clearly that one thread of implant is exposed on distal side, it means the implant not buried properly from the first time and lead to bacteria colonozation on implant surface
Having only placed a handful of lower second molar implants I don’t have the sample size to reach statistical significance but my observations would suggest that they just have issues of unknown origin, just like second molar teeth. I think every person who has posted a potential reason for this failure is correct but I also think the most likely explanation for this case is S&#t happens. I was taught that a fully intact occlusion was 2nd molar to 2nd molar but over 85% of a person’s chewing function happens 1st molar to 1st molar. On top of this the human body has an amazing ability to compensate for 20-25% loss of function to reestablish 100%. If this is true, and I have found it to be at least consistent, then a single mandibular second molar accounts for 1/4 of 15% and it resides in an area of difficult access for both the patient and the doctor. Certainly there are exceptions but as a general rule patients get very little in return on investment when we place a second molar implant…
Look at the work of Dr. Greg Steiner by going to Steinerbio.com for a possible clue. His studies show that allograft results in sclerotic bone. It is essentially scar tissue. It appears normal and very hard when the implant is placed. But it is not able to remodel well because of lack of osteoclasts. This implant was placed completely into a socket that was grafted with allograft. Add 3 years of stress on this 2nd molar. Goodbye “bone”?
For the last 2 years, I have been advocating to my associates to use only Steiner’s Socket Graft/Immediate Graft for socket preservations and immediate implant placement, and Ridge Graft for large sinus grafts. Our experience has been very positive. The graft is a formulation of beta tricalcium phosphate.[quote="Daniel_Camm, post:17, topic:1329, full:true"]
Look at the work of Dr. Greg Steiner by going to Steinerbio.com for a possible clue. His studies show that allograft results in sclerotic bone. It is essentially scar tissue. It appears normal and very hard when the implant is placed. But it is not able to remodel well because of lack of osteoclasts. This implant was placed completely into a socket that was grafted with allograft. Add 3 years of stress on this 2nd molar. Goodbye “bone”?
For the last 2 years, I have been advocating to my associates to use only Steiner’s Socket Graft/Immediate Graft for socket preservations and immediate implant placement, and Ridge Graft for large sinus grafts. Our experience has been very positive. The graft is a formulation of beta tricalcium phosphate.
The subject of bruxism is quite interesting. We did a quick search using OsseoNews AI and created a new post about it with the top references: Does Bruxism cause implant failure?