Hello docs,
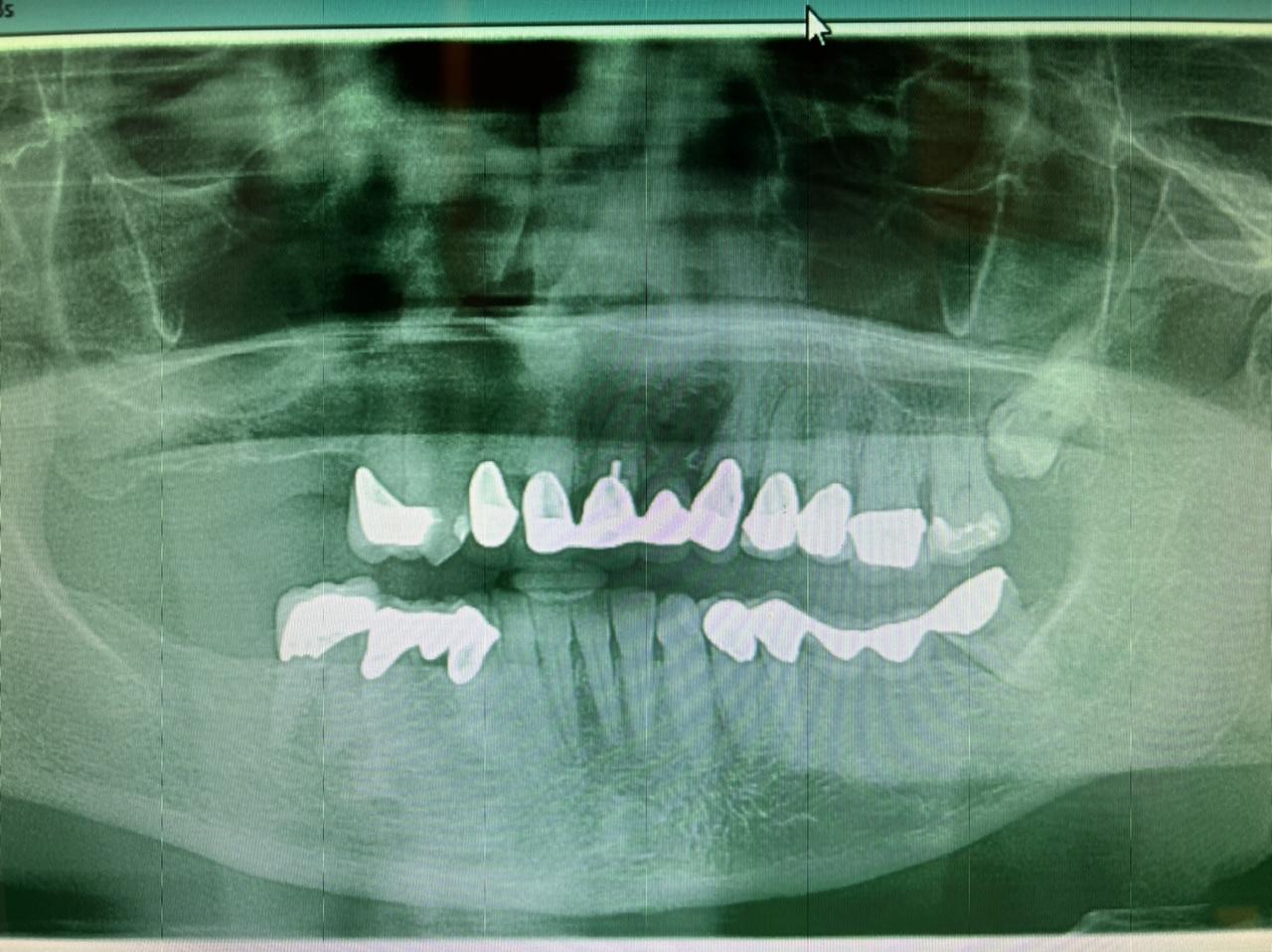
I am feeling really humble. I’ve placed multiple implants and thinking this should be a straightforward case. I was wrong. I know it’s poorly planned and freehand did not go well. Are these restorable? Should I explant and redo? If I do remove these, how easy is it to remove these?
Please CC’s only.
Thank you in advance
Dr K G comments:
If they are no integrated, I would take them out and put right. Also check for secondary caries under 3.4,3.5
Dr. Humble comments:
I placed them yesterday. How easy would it be to remove them if they come back on Monday for Explant? And what steps should I take?
DeeR GeeSin comments:
theyll come out easily. just "unscrew" them. do it the right way. the pt deserves it AND will appreciate it. "mr jones, Im going to remove one of the implants. After studying the xray I dont like its position and i know I can do better. unfortunately were going to lose some time up front(if youll need to bone graft) but in the long run we'll have something thats closer to perfect". time to eat humble pie and admit you could do better. patients always apreciate that.
Richard comments:
Get a CBCT. Angled heads might help. However, my concern even if you can restore these two implants is the encroachment o[nto tooth #20. What's the possibility of a devitalization of #20 from the implant next to it? Might need to do an intentional root canal on #20. This one radiograph itself is not enough information. You also need a study model. Also, would you need to place another implant to engage the occlusal surface of #15? The freehand placement angulation leads me to think that you are right handed.
Dr. Humble comments:
Yes You are correct, I am a righty. I placed these two days ago how easy are they to remove after 4-5 days of integration? Bone did not feel too hard when I was doing osteotomies
Richard comments:
Addendum: #14 is extruded past the occlusal plane. Need a new crown on #14 and shorten #15. Do you have immediate cuspid rise bilaterally? #15 probably has bone loss on the distal in relation to the impacted #16. In other words, this case needed more analysis before committing to the implants.
Dr. Humble comments:
Yes I agree. Patient had an existing long span bridge which #17 failed due too crack and decay. I sectioned the bridge and took 17 out and placed these two implants
Dreamdds comments:
Even if you try to restore I feel you will find the impression posts will not seat due to acute angle. Even severely cutting posts and if the impression does index the platforms, the lab will be severely hindered and they should send the model back and not join in the liability loop
We have to understand we place many limitations on case for lab to restore.
Good luck be honest with patient and make them whole
Leonard
Dr. Humble comments:
Thank you for the advise. How would you go about explaining the possible complications with the patients? Given that these are still restorable with difficulties, inform patient about possible RCT or EXT on #20? Thank you
FM comments:
So these two implants are to receive a crown or two crowns opposing the upper first molar? For starters please don’t cantilever behind the second implant.
These are restorable btw but with a bit of a fight. Shorten the impression post or use a regular sized shorter abutment, so that it doesn’t collide with the post of the second implant and transfer free hand. There after use an angled abutment as the definitive. Can always let the first implant sleep and do a teeth and one implant supported 4 unit bridge, If you are totally out of other options. I don’t think removing these would be easy if they’re integrated well.
Dr. Humble comments:
Thank you for your advice,
These were placed yesterday and it was my fault that I had my DA take the final PAN and patient was dismissed. I shouldve checked the PA before finishing it. How easy would it be to remove at one week follow up or even next Monday? I planned on scanning these implants with scanbody one implant at a time which will give me some room to fit two scanbodies. Thank you for you input!
Barrow Marks comments:
Take my advice and this case will be easy. And if you have a scanner even easier.
Take an impression of only one implant. Then take a separate second impression of the other implant. Send both impressions to a lab that can scan both impressions. The lab should have software that can knit the two impressions together and mill two custom abutments and splinted crowns. Even better if you have a scanner, take a scan body impression of one implant then remove that scan body and place it in the other implant and do a second scan of the second implant. And the lab can do the rest. You can even do one scan if you place two scan bodies and trim them so they can be seated. But you must redo that upper molar crown or the occlusion will ruin your masterful work up to that point.
Dr. Humble comments:
I appreciate your advice! I do have a scanner and I have been scanning with scanbodies to restore my biohorizon implants. I never placed two implants closed together like these so I was concerned. I wasn’t able to put two healing abutments side to side together either. But listening to your encouraging comments and helpful tips I gained more confidence. Thank you Doc!
Barrow Marks comments:
Also please avoid an explanation. Those implants that you placed so well look well integrated and given their angulation with be very destructive to remove. I would rather see you put one to sleep then go that route. You did a good job in spite of your fears now you can complete this case and we can revisit your work in 40 years to celebrate how well it was done.
Barrow Marks comments:
Sorry I didn’t realize that these implants were placed just a few days ago. Explantation will be easy just reverse torque . But follow my comments and none of that will be necessary
Tim Carter comments:
I think you have options here. You could leave them both and restore 19 only and worse case scenario 18 could be used in case of failure. You could follow any of the suggestions offered to include removing 18 only as it should be easily reversed within the next 3 weeks. One thing that the radiographs suggest is that the patient likely has a thick lingual shelf of bone supporting thick soft tissue. This possibly limits your ability to properly place 18. As suggested earlier address 14 PRN.
Dennis Flanagan DDS MSc comments:
Get a CBCT to demonstrate the exact positions.
Rob korman comments:
I agree with Dennis F. Take a CBCT to figure out your surgical and prosthetic parameters. You will have potential esthetic issues if it’s in the smile zone as well as potential hygienic issues if you restore with present implant position.The PA reveals inadequate room to develop interproximal tissue. As you know, you need a minimum of 3mm of space between adjacent implants to predictably develop interdental papilla.TAKE A CBCT!
Dr Pravin patel Mumbai in comments:
It's simple case..put direct abutment of appropriate direction..mill intra orally and make it little rough( just remove shining and scan...you can go ahead with cement retain crown ... There is definitely more spacing intra orally than what visible here..put healing abutment..customise if not fitting both together
