Help I’m not sure what implant system this is. A flat coverscrew maybe placed about 20 years ago. Can anyone help identify it ?

This could possibly be IMZ
Thank you for your input the flathead coverscrew doesn’t span entirely across the width of the cover. Having looked at IMZ components it appears they span the entire diameter.
is there another on the lower left? was this supposed to be used for an implant retained lower partial denture? if not, just remove it. no point restoring an unknown implant. with so much bone loss is it worth restoring?
I’m not looking to restore it. The healing abutment is tall and I was planning to unscrew it so I could hopefully submerge the implant. Explantation isn’t an option unfortunately.
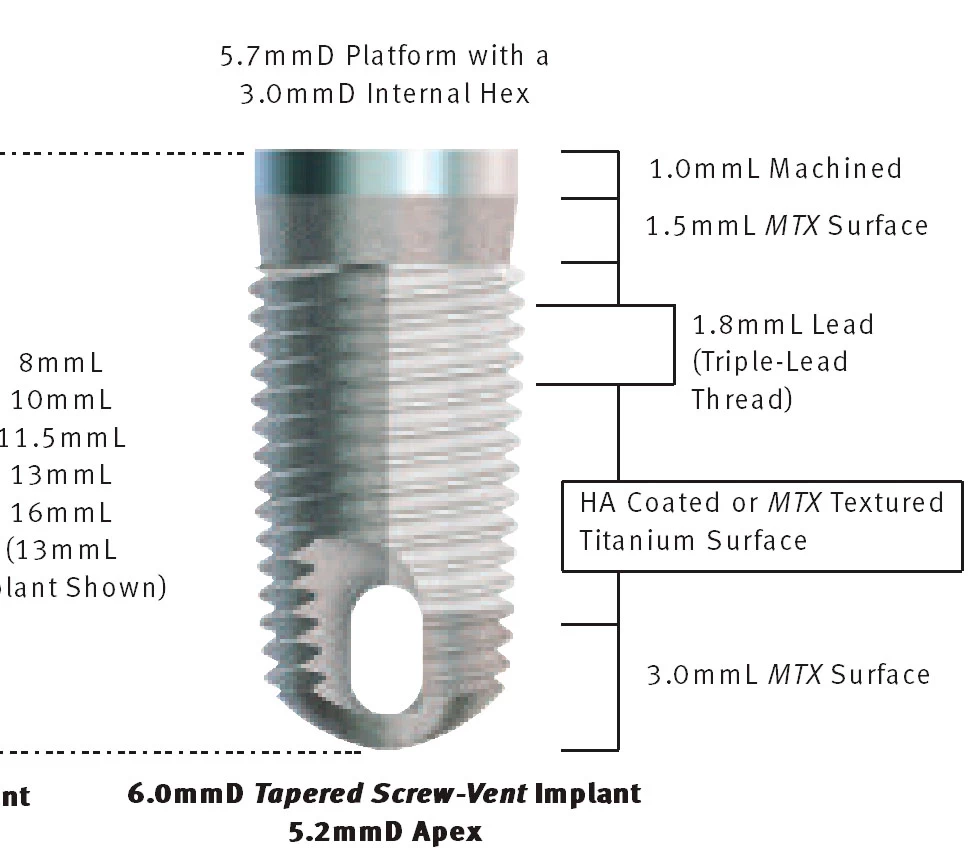
The picture reminds me of one of Gerry Nishnik’s old ScrewVent or Corevent fixtures. I also thought IMZ (same era of implant designs)…
if cover screw already placed. there is no healing abutment. you wont be able to “submerge” or bury it. its already “submerged”. the implant is “tall” because there is 50% bone loss resulting in exposed implant.
the cover screw by definition is at platform level already. you can’t make the implant “shorter”.
Thank you for your input. Apologies for my lackadaisical terminology, having completed some non surgical work in my opinion it’s currently a healing abutment which can achieve some reduction in height with a coverscrew instead. What are you thoughts on burying a failing implant if achievable, i anticipate no more bacterial ingress and therefore a dormant implant ?
what is the country of the implant? Couldn’t it be Straumann?
Or could it be Biomet 3i?
take some I/O photos and post here. better to evaluate from our end. but from PA. looks like you have cover screw NOT healing abutment on the implant. nothing you can do more to change the height of the implant.
if the implant is exposed its exposed. you can only remove it.
if implant not exposed. then just leave it be and relieve the intaglio of the ur RPD at that site. so the RPD doesn’t hit the implant and cause pain on the gingiva.
Could be an old Calcitek, which was taken over by Zimmer a long time ago. They were HA coated cylinders.
I would be surprised if this is anything other than Core-Vent/Calcitek/Zimmer… all the same. It is certainly shaped like a Zimmer and it has what appears to be the signature hole at the apex of the fixture which is still the signature of ZimVie, formerly Zimmer, formerly Core Vent etc…
Its difficult to tell for sure but is there a retained root tip on the distal of this fixture???
Not not a retained that I’m aware of.
I’ve managed to get some further information/clinical notes apparently this implant had caused sepsis in the past and was advised for removal in a hospital setting. Alas I still search for the clinical notes for which implant was placed but I’m getting closer. Thank you for everyone’s feedback.
The question that I still query assuming it is not a healing abutment and I can disinfect and submerge with a coverscrew is that a legitimate option. Any evidence in submerging failing implants ? Further infection or ceasing bacterial ingress ?
dear dr. dont think your reading my replies carefully because you are repeatedly asking the same questions about submerging the implant. this implant already has a cover screw. You can’t “submerge” the implant, technically the implant is already “submerged”. you can’t change the height of the implant. Is there a reason you can’t remove the implant? why need to be in a hospital setting? what medical issue does the patient have?
if your implant is exposed then bacteria is all over it and building biofilm. you can’t remove the biofilm and there’s no way to disinfect the implant.
Dr teng, I appreciate it looks like a coverscrew and certainly that’s what I also initially thought but on closer inspection disinfected with magnifying loupes it appeared to actually have a healing abutment. I will confirm in due course and take photos, I believe the angulation of the radiograph doesn’t help.
History of oral alendronic acid but I understand this is not an absolute contraindication. Also simply doesn’t want it out very anxious patient. Possible close proximity to mental nerve but will take a CBCT.
Besides what I’m asking about submerging is now a theoretical question rather then for this unique case.
modern implants if you see threads by the platform of the implant. then it’s a cover screw. If you see smooth metal around the circumference. then it’s a healing abutment. this patients implant surface looks all smooth on the PA (could be due to angulation of your PA). but at the platform you can see the cover screw threads inside the implant plus you can see the outline of the cover screw at the platform. that’s why i agree with your initial assessment, the implant has a cover screw and not a healing abutment. Get a universal driver kit on ebay. im sure one of the drivers can remove the possible “cover screw” then you will know exactly what’s placed on the platform of the implant.
h/o Fosamax is not contraindication to removal. any osseous surgery will have risk of MRONJ. if surgery is necessary that’s the risk you and the patient take unfortunately. hopefully you won’t have complications. Also even without osseous surgery, MRONJ can still occur spontaneously for patients taking Fosamax. if you look up AAMOS MRONJ position paper, "The data suggest that antiresorptive medications (i.e., BPs and DMB) are associated with an increased risk for developing MRONJ. The risk of MRONJ is considerably higher in the malignancy group (<5%) than in the osteoporosis group (<0.05%). " so rate is very low.
if its #27 or 28 site then you are far from mental nerve. not even a risk in your case, unless you trephine extra deep and way distal to your implant during implant removal.
of course you can bury a bone level implant. all “bone level” implant can be buried with a cover screw and exposed with a healing abutment during 2nd stage surgery after implant integration. In this patient’s case, perhaps the implant was bone level at placement, but it’s now a tissue level implant due to the bone loss. also you can see calculus on the implant.
if you are not going to use, remove or restore the implant just leave it then. Just design the RPD to not touch implant site. But if there’s erythema, swelling and pus expressed then implant should be removed regardless of Fosamax use. because constant inflammation/infection at implant site is not good for pt taking Fosamax either. If MRONJ does develop you will lose that implant anyway, plus necrosis of the bone at that site, and necrosis can spread.
Good luck.