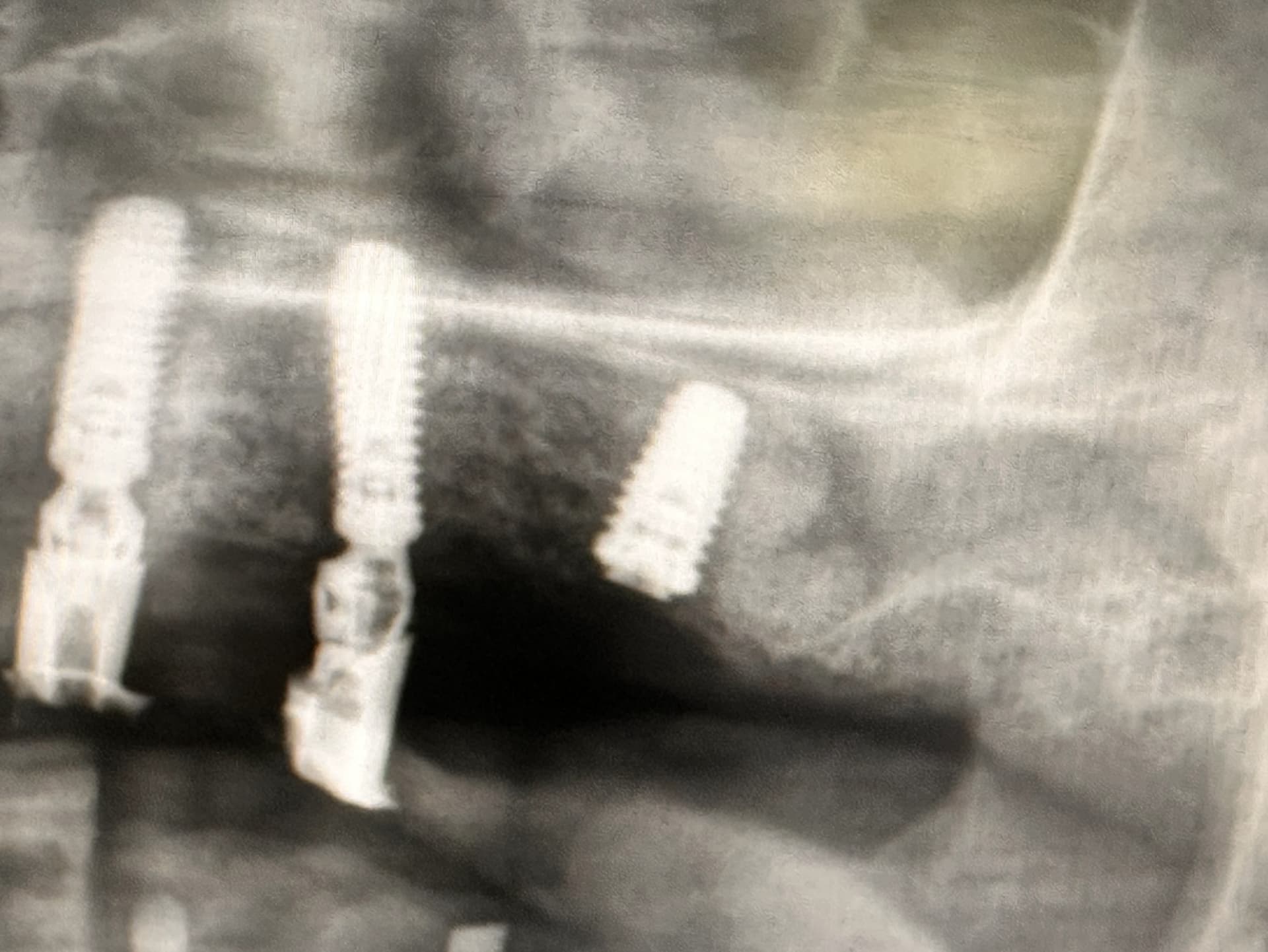
Does it look like the sinus membrane is perforated?
The CBCT was taken immediately after the surgery.
The patient has had no sinus symptoms two weeks post-op.

Does it look like the sinus membrane is perforated?
The CBCT was taken immediately after the surgery.
The patient has had no sinus symptoms two weeks post-op.
It is possible though I don’t think it matters. When taking out upper molars we perforate sinus membranes all the time and it doesn’t matter so an implant fixture piercing the membrane while also sealing the hole should be just fine as well. While I would not suggest we intentionally put implants into the cavity I have been allowing them to go 1-2mm into the sinus for years as a way to achieve bi-cortical stabilization and no issues… This should be just fine.
So what is the treatment plan? Why was the implant placed?
it’s part of the AOX procedure
Just out of curiosity why did you select this position for the implant if it was part of an All-on-X? It would appear from the selected images that a more appropriate site exists distal to the chosen site and to the best of my knowledge all-on-x relies simply on multiple fixtures spread out with cross arch stability so the distal site might be more appropriate. I don’t think it will have any bearing on the future of this case but it would make for one less potential stressor.
No. It doesn’t look like the membrane is perforated. When we graft the sinus the lining gets inflamed and swells. This will disappate so when I do a lateral window sinus graft ( Caldwell luc), I Rx a Medrol dose pack.
Contrary to what others have said above, the rough surface of an implant that perforates Schneiderian membrane, is a great nidus for bacteria. it can cause a chronic sinusitis. Ask me how I know. Yes, I too have perforated the sinus floor without consequences. I will generally now put L-PRF to help the body repair the membrane tear. Good luck.
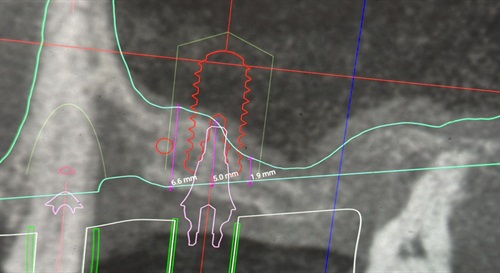
kinda strange. for AOX. usually the implants are placed anterior of sinus in the premaxilla area to avoid sinus lift. or if when there’s not enough bone in the premaxilla to support implants, paranasal, zygomatic and/or pterygoid implants are used for more advanced AOX. If i were to plan for AOX with implants placed at sinus location (which i have done before, because patients sinus were very anterior and there’s just not enough space for 6 parallel implants in the premaxilla area) i would have performed sinus lift also. just to avoid future problems. for AOX i wouldn’t want any implants to have a chance to fail. Even in your CT planning. 1/2 of your implant (>2mm) is in the sinus. Why would you take this risk for future problems? for your AOX case. this distal implant failure could mean new prosthesis. Which would have been avoided if you did a sinus lift. And with sinus lift you could have placed a longer implant.
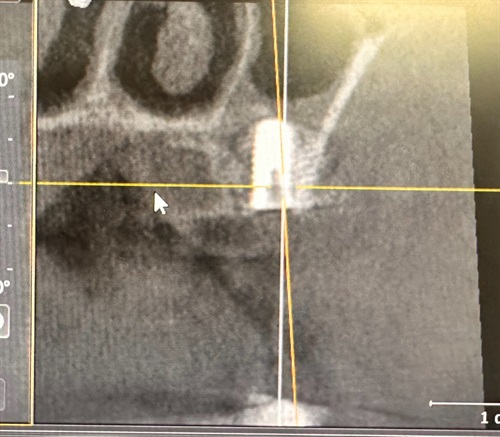
also I’m sure when you performed the osteotomy the sinus is perforated. sinus membrane heal very well due to good vascularity. just because you perforated the membrane doesn’t mean you will get a sinus infection or have symptoms. im sure pt was on antibiotic pre and post surgery. and you inserted a sterile implant to occlude the osteotomy. you just cannot really evaluate the sinus membrane on the CT post op. the implant just causes too much artifacts to definitively say otherwise.
the question will be. when this implant fails. and you need to redo the denture. would you kick yourself in the butt thinking. “i should have grafted” or “hindsight is always 20/20”
if it’s a single implant/crown. i wouldn’t care less. but an AOX is a different beast.
I don’t understand what meant. The sinus lift was performed.
Did you do a vertical or lateral sinus lift? If after you did the lift and saw the membrane intact. Then sinus is intact. From the PA. The graft formed a nice white bubble. If the membrane was perforated. U would not see that on PA. I’m gonna guess u did a vertical lift with versah burs?
This is a great topic for discussion and we used our AI to generate a summary of all the latest research, Sinus Membrane Perforation: Risks, Repair Techniques and Implant Survival. In reading the comments, I think Scotty’s initial thoughts are most in line with the research we found.
With this limited X-ray data it seems there may be a horizontal fluid level in the sinus; can you compare your cbct prior to implant placement? Just many variables to consider
@gregkammeyer gregkammeyer, For the same procedure, if the sinus membrane is perforated, what would be the main difference in appearance on an X-ray or CBCT compared to this case?