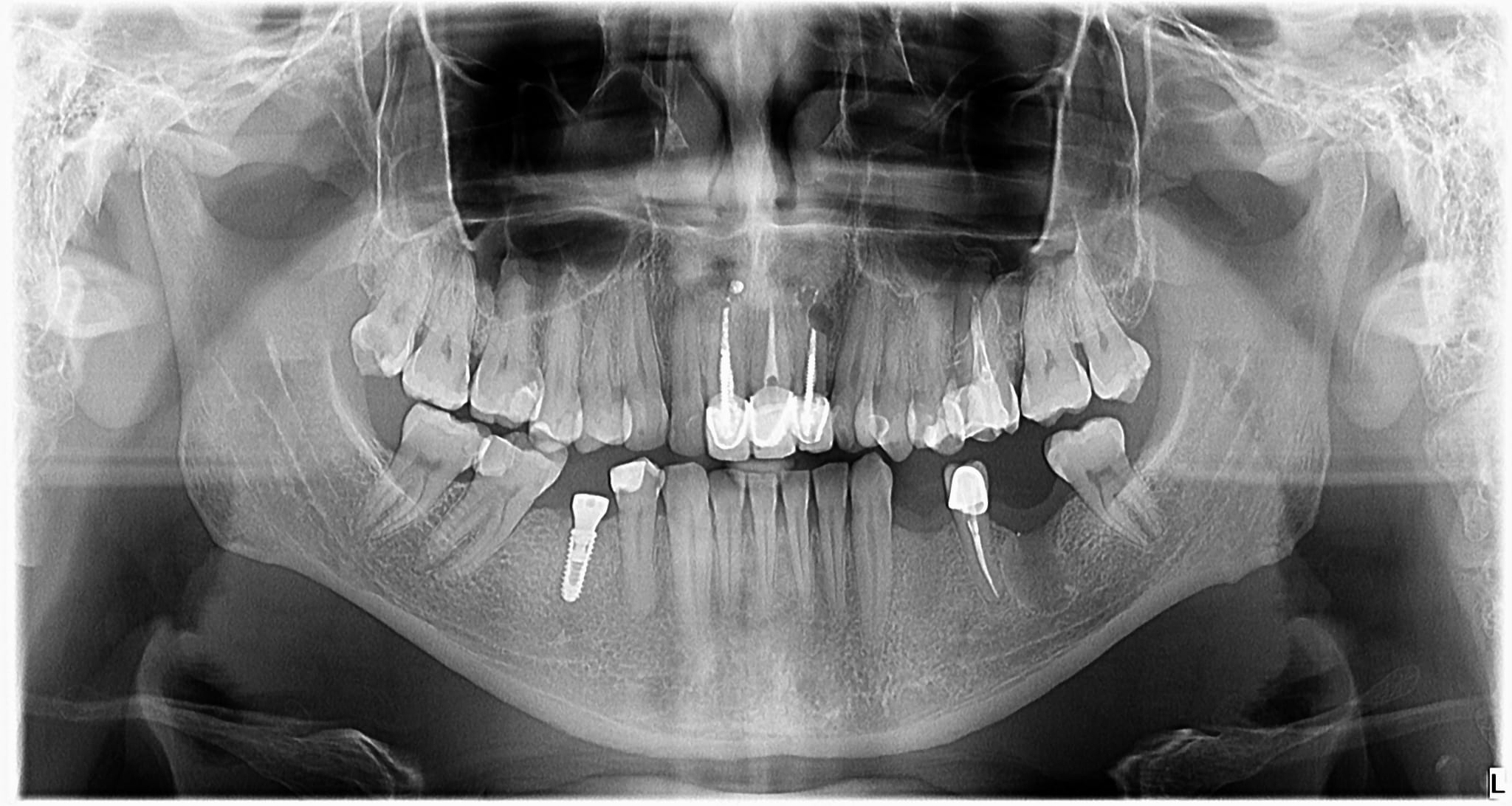
I have a new patient, that was referred from another doctor. He said that the cyst was removed 4 months ago, from the tooth 36. I placed a month ago, one implant în the 4th quadrant, and now I want to put implants in the 34, 36, position. But I don’t like how it looks, it seems that the cyst was not removed correctly? Or it’s not healed? It’s a 40 year old Male, healthy, but heavy smoker. What would you do?
I think it has fully healed but with a residual scar. Since it has been 4 months since the extraction I would proceed.
Open it and you will know. It will be an implantation weather an exploration. What could anyone else do, have better grayscale vision?
it’s most likely an PA abscess/granulation tissue, not cyst that was removed. Since no BG is placed. the socket looks radiolucent. unless demineralized allograft was used which show up radiolucent also. if pt is a heavy smoker. you can wait another 2 months for bone to consolidate. you can definitely try at 4 months post extraction. but i bet its still soft bone. You probably just use couple drills short of your implant diameter. extract upper 3rd molars while your at it. good luck
1 Like
Listen to your gut. I don’t like how it looks either. Probably benign but distinct radiopaque defined border. If things go sour you will need to currette the lesion, possible biopsy. Are you prepared? It’s sitting directly above the IAN. If you had a CBCT you could see how close. A pre extraction pa would’ve been helpful. It’s (36) not your problem, share the liability and let an oral surgeon deal with it and site prepare, then it will go as easily as 45.
Listen to that little voice that is telling you to go carefully.
Why not place your implant in site #34 and at the same time extend your flap slightly to the distal of #35 and visually see the quality of the bone on the ridge above the healed socket site. You can also contact the previous clinician who removed the tooth and find out a bit more information.Waiting another few months for the bone to densify more is not such a bad thing
Look at the UL lateral incisor (10)… I assume the tooth that was #19 had a PARL which possibly healed in a similar fashion which leads me to believe that while not normal it could be a variation of normal for this particular individual.
You can’t go wrong if you or an oral surgeon opens the site and take a core biopsy, currette it and see if it’s soft and if so submit that too and then add some bone and close primarily. CBCT would be helpful and you could limit it to the mandible and do that before anything else…no smoking postop to be stressed
Get a CBCT scan and go from there. I always want a scan in this region to know ridge width, cross sectional shape of the jaw from top to bottom(is there a large lingual undercut?), and location of the nerve. You can answer all anatomical questions with a scan and treatment plan from there before launching into step one of treatment.