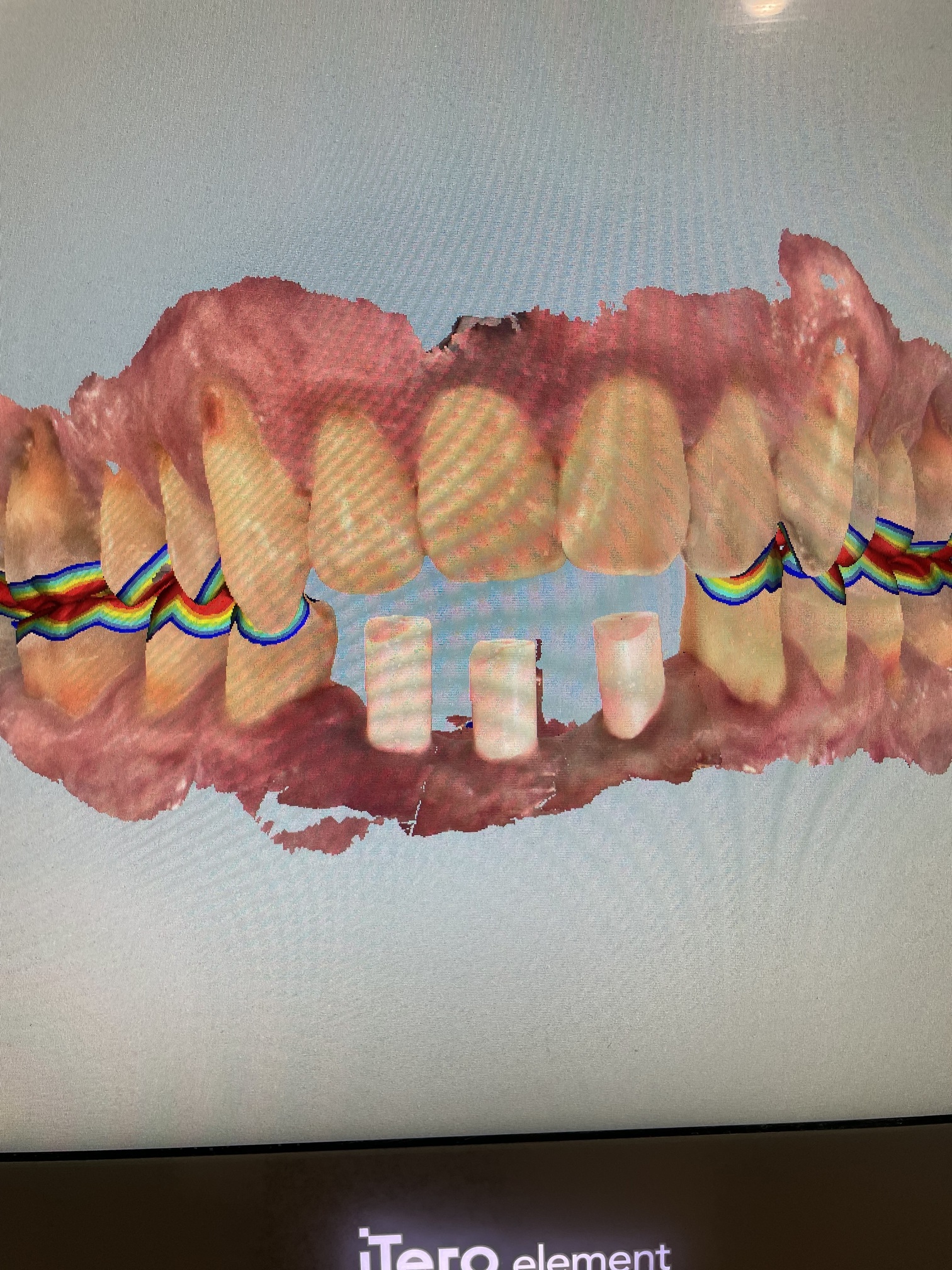
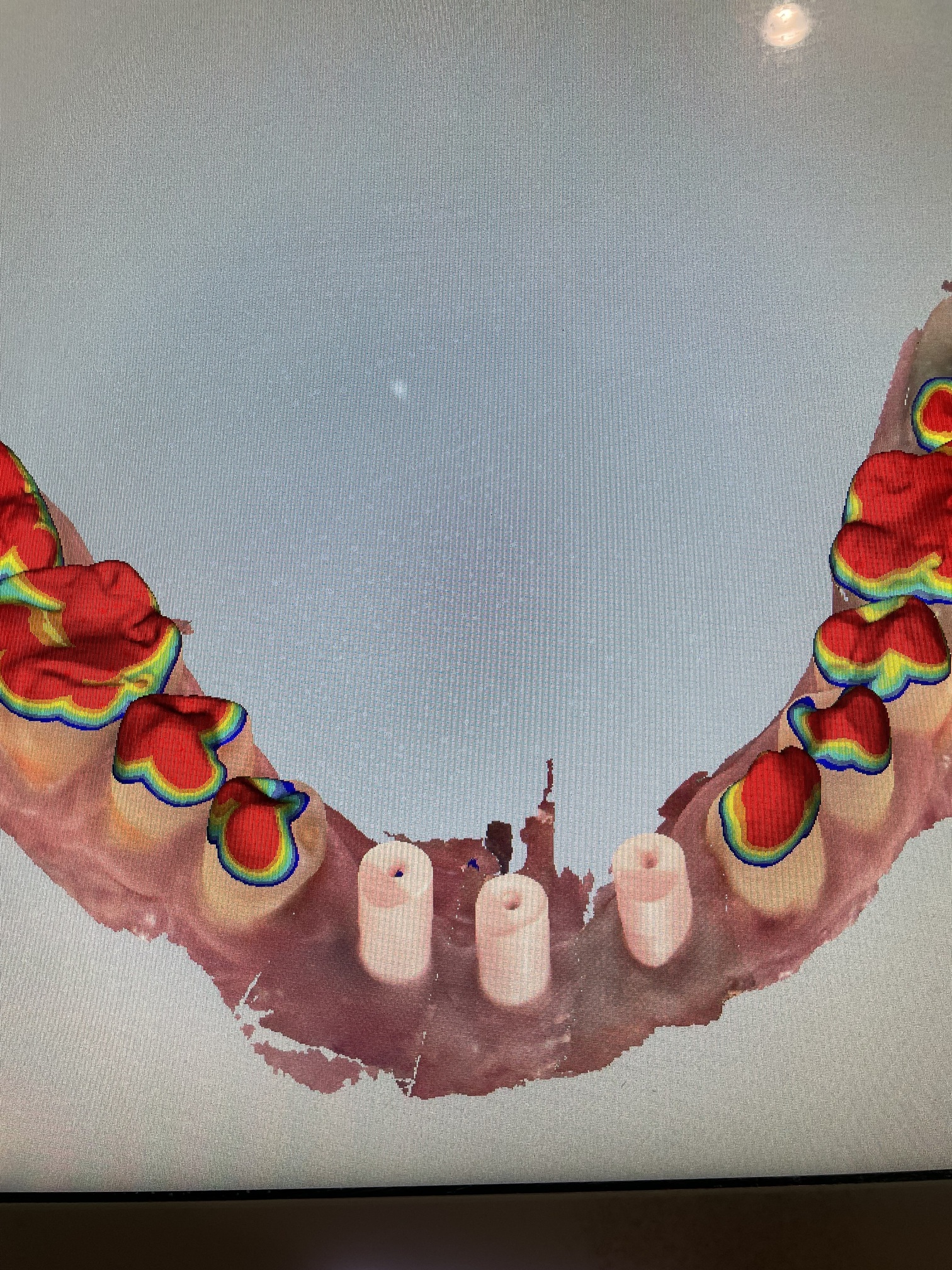
I was sent this case by an oral surgeon to restore. The patient had trauma and lost his 32-43. They grafted and placed three implants. He has an anterior open bite. I’m hoping to do one large single unit screw retained restoration but unsure what material would be best. Or any other recommendations? I haven’t come a case this big before, as normally I’m used to restoring 1-2 single tooth implants.
Thank you
Dear Mike, Since this should have been waxed up prior to the implant placement allowing for a prosthodontically driven implant placement; I would ask the oral surgeon if they did this. Also you may ask them to consult you for wax-up and planning in the future prior to any implant placement. You will need to purchase impression copings and request a diagnostic wax up and laboratory fabricated provisional to work out occlusion, address the anterior open bite and see if you will have an acceptable esthetic result. This is a separate fee and then you can, if acceptable, provide a definitive restoration. Note: This may need to be cement retained if screw access is not desireable. If the screw channels are in embrasures, then you will need cast abutments and a cemented bridge. I prefer PFM bridges for any cemented restoration with titanium abutments. I hope this helps. Rick
Hi Mike, you can sleep the middle implant and do a four unit bridge. Screw retained allows you to remove if needed in the future. Occlusion will not be an issue due to his anterior open bite. This may be an option vs restoring the three implants with limited restorative space.
1 Like
Thank you very much!
At this stage send it yo your trusted lab tech and discuss the restoration with him/her first. See what is possible and best for the situation. I think you will be able to use screw retention which is certainly preferable for a variety of reasons. in a situation like this I would typically place two implants closer the the neighboring teeth and restore using a bridge. Since the middle implant is already in place and looks good I would go ahead and use it if at all possible.
Screw retained on multiunits if implants are positioned good enough.
He has digital impressions with scan bodies. What you suggest can be done with the information he has. No need to go backwards to analog.
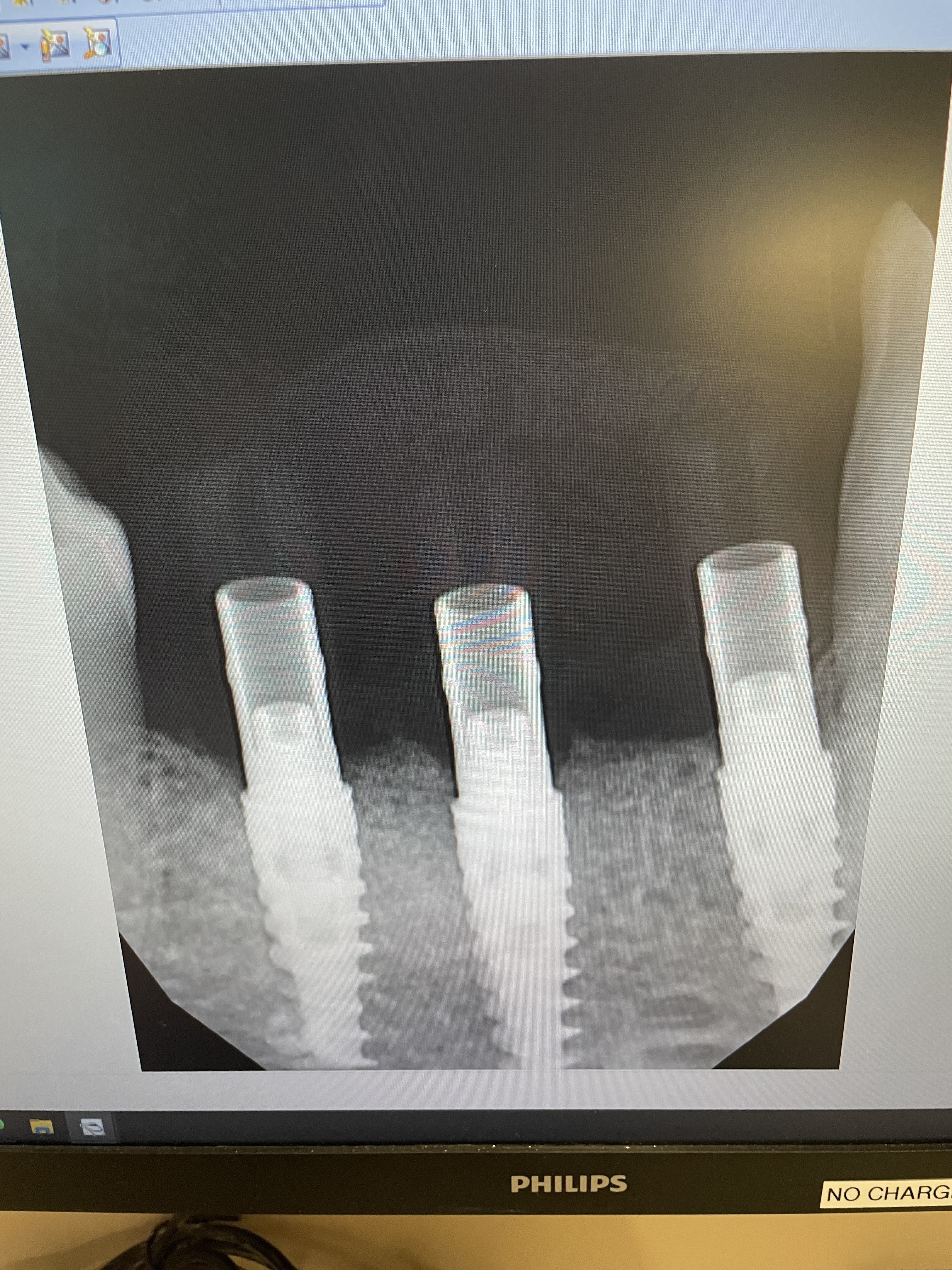
My lab looked at the case and proposed three separate screw retained units ( 43/42 cantilever, 41 crown, 32/31 cantilever). They said given the path of the implants, one large screw retained unit wouldn’t be possible. They suggested zirconia as have done cases like this in the past.
Does this sound reasonable?
IF you place these as separate units, you increase force factors. You create a cantilever that also is a force magnifier. Using a provisional and taking PEEK abutments and a cemented provisional will allow you to work out if cosmetically it’s feasible. There is nothing wrong with this being a cemented bridge. Ideally the implants would have been put in terminal implant positions with the central implant coinciding with one of the pontics. This was not done. So now you have to bat clean up. To do this it may be best to work this out with a provisional prior to completion.
Most likely this will be an easy case to restore. I agree the with first comment about prosthetically driven or “crown down” design. Surgeons typically place implants with little regard to restoring them. I think the dentist should be the “quarterback” of this team. Whether you do a wax up first or if you have the capability to scan and design first then it is a simple matter to place implants with regards to the prosthetics- “crown down”. The dentist tells the surgeon where he wants the implants based on the prosthetic design. Hopefully the alignment will be good and the screw hole won’t be thru the buccal or incisal. If it does, then an angulated screw channel (ASC) might be utilized. If it comes out between the proposed teeth in the interprox area it’s not the end of the world, but that’s why you learn about how the design dictates where the implants should align. My favorite statement is “don’t do the first step till you know the last” is an homage to careful planning. Of course the longest journey begins with the first step. Since you have access to a scan with 3 scanposts seated, just forward that to the lab with a shade and they should be able to give you a finished product. I don’t think you need to drag it out with a Peek temporary. The open bite makes your life easier too- no occl to worry about. (Provided the patient’s expectations weren’t to close the bite to start with, in which case maybe you can reduce the openbite, otherwise ortho should have been part of the initial discussion and in the informed consent prior to starting). Also, if the patient paid for 3 implants, his expectation would be to utilize all 3, otherwise why would he have paid for it. It still seems to be a straightforward design. Make sure it’s passive on seating. Engage torquing a little bit on each one, alternating till you get to final torque. Good luck.
1 Like
Dr. Holden, 3 separated screw retained crowns are a good solution. You might want to use pink porcelain in the gum area.
I would wonder 2 things: do you have a PA x-ray that separates the patients LL cuspid from the implant? What is the cause of the anterior open bite? If it is long term and stable than it’s safe to proceed. If it has developed over time then there could be joint damage/degeneration, intra-arch changes or inter-arch changes. Spears has a module on this topic. You’ve been given lots of great advice. I note that if you are to cantilever the splinted units they will take the forces better, esp if it’s caused by an inter-arch problem. Good luck.
1.Don’t worry about esthetics. Nobody’s going to see it.Pink porcelain is feasible
2. Worry about retreivability. Do screw retained and 3 separate crowns
r