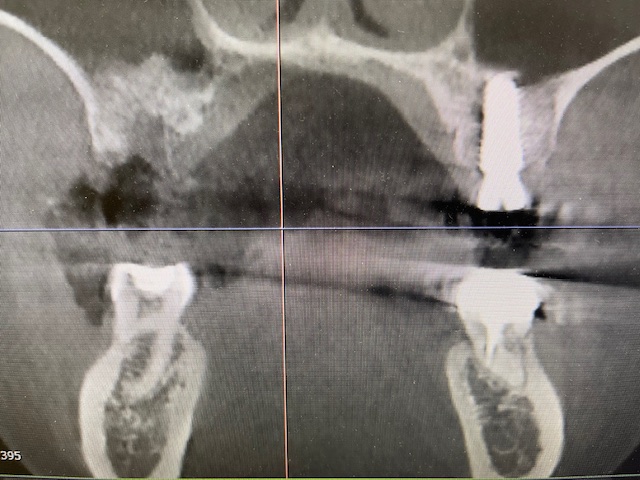
couple days ago, performed an implant placement at #3,14 site for one of my dental assistants. Teeth #3,14 were previously extracted and grafted due to pain and failed RCT. I forgot #3 site only have 5mm of sinus floor and osteotomy through the sinus floor. which was indicated by the parallel pin in CBCT. I quickly placed a 5x11.5mm Hiossen implant at #14. and proceed to #3 site. I used Versah burs applying crestal sinus lift protocol 2. which formed a nice white bubble on the sinus floor which i subsequently placed also a 5x11.5mm Hiossen implant and placed a healing cap and buried the implant. So far pt seems to have normal course of post op symptoms.
Although i perforated the sinus membrane, it is still possible to continue with a crestal (vertical) sinus lift and place an implant. However, i still placed pt on PO abx (augmentin) whether i perforated the sinus or not.
I have a question regarding the use of radiation as it relates to implant dentistry. I know that I am old fashion and while I wouldn’t recommend it I still do the vast majority of my cases with only 2D radiographs despite the fact that I have a wonderful Carestream 9600 CBCT machine in my office. It seems like a lot of folks take a lot of CBCT images in conjunction with their implant cases and I am curious at what point is it too much. I am well aware of the minimal amount of radiation from our equipment but the smart people on the national news that so famously mislead the American people will caution against all of this. How do you explain/convince your patients that all of these images are necessary, even if they are, how do you justify the exposure to a skeptic when the end goal is nothing more than a screw in their head which isn’t necessary in the first place. I guess I have just encountered too many people with too many questions for me to be taking multiple CBCT images for the purpose of placing a screw…
Thats a great question. as you know. since Feb 2024, ADA has abolished the use of lead aprons/collars (please read ADA guideline). I don’t think patients have a choice in radiographic preference. I take images as needed. for example, for 3rd molars removal. i can use PAs but i prefer PANO (instead of 4 PAs if all 4 were taken perfectly which is usually not the case. then pt is exposed to more radiation for retake). because PANO gives a more accurate picture between impacted 3rds and IAN. If your office dont have a pano and you use a PA thats completely reasonable (since pano/CT are not standard of care for 3rd molar images). But, if i get sued and i dont have the proper images to back up my clinical/surgery decisions. I will be cruxified by experts/specialist like yourself.
Sinus grafts are difficult to get a clear picture on PAs, bc sinus is much wider than alveolar ridge. I prefer a CT scan so i know and pt can see that the graft is consolidated and around the implant which protects me (like good documentation) from any kind of unforeseen complications and i can educate the patient. there’s no point for needless risk only to avoid certain imaging. If you have CT might as well use it to its full capacity. But if im placing an implant in the mandible or max premolar area, i just take a PA like you. unless at consult, during clinical exam, i have doubts about alveolar ridge dimensions and need GBR.
During mission trips overseas, i’ve remove teeth w/o imaging all the time. which proves you don’t need imaging to remove teeth. Doesn’t mean that’s a good thing, that’s only because of the limited resources in 3rd world countries.
In conclusion, if i can get away with a PA. i would. if not, i’ll take PANO or CT (sometimes just easier for your assistants to use PANO/CT. i doubt you are the one placing the sensor and beam and pressing the button) and if patients tell me otherwise. I usually tell them I’m not superman and don’t have xray vision. so i need to take whatever images i need. if they refuse imaging, they are welcome to go somewhere else. bc images protects the patient and us, clinician.
Many of my patients are sedated during treatment and it is not practical to transport them to the CBCT machine. Perhaps the environment has shaped me to rely less on imaging since the condition of the patient doesn’t support it…
I would say your case went very well. The slight perforation will probably be ok because you did not extrude a bunch of foreign material into the sinus for her body to deal with. Implants into the sinus less than 4 mm can be tolerated well. That being said a 10 mm implant could also have been chosen , even an 8.5 and you would not be addressing this situation. Some would “repair” or plug the perforation with collagen and or prf and place the implant. Some would abort placement, plug osteotomy with collagen and or prf suture and re-enter the site 6 weeks or 4 months later. Always use antibiotics. I would suggest you obtain pjlebotomybtrainingvatvanlival community college and add that to your skill set. I have been involved with L-prf for years now (20+) and it makes a substantial improvement on your patient recovery and your treatment successes.
When I did my master’s research on bone grafting, I had to go before a university radiation committee, (alot of MD’s) as I used 3 medical grade CT’s in 6 months. Given the radiation from those images is 30x what our CBCT machines have and that with my Carestream machine, I can take a 5 x 5cm image to focus on the area at hand, I am totally comfortable with the amount of radiation. Esp on Caldwell luc antrostomies, as the width of the sinus determines how long it will take for the bone to turnover, what are the pathologies/sinus webs and how much bone will be needed.
From a professional point of view, I wonder why you wouldn’t want the image? Less distortion shows 3-D anatomy and helps me truly see, before surgery the true site and After I do surgery, exactly where the implant wound up. This is humbling.
Scotty, I get where you are coming from. I too used pano’s and PA’s when I started implant placement in 1985. After 14 years of using CT’s on ALL new patients, I don’t know how much quality I’D sacrifice if I was using 2D. Alot, I am convinced.
I’ve been told that a new CBCT machine radiates about the same amount of radiation as a cross country flight.
If you believe it’s in your patient’s best interest either way, that is what they will follow.