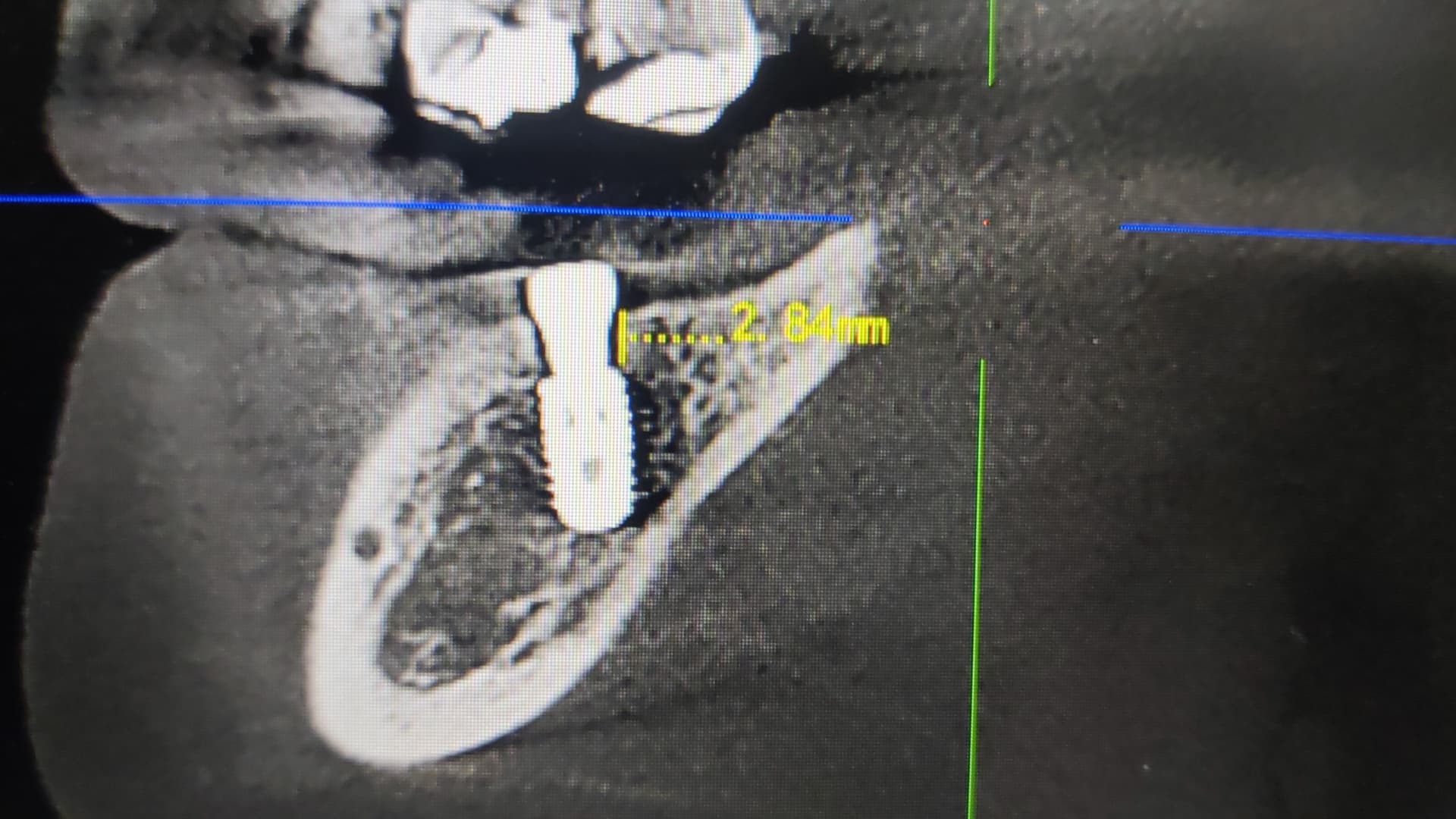
Hi. My implant planned is 5.0mm/8.5mm I drilled with 5.0mm/8.5mm implant drill ( with surgical guide) my implant was placed 3mm subcrestal. Just yesterday. It is quite near to the ID canal. And I placed healing abutment (because I used tissue punch)
Do you advise me to remove it and place a slightly bigger implant( but that would be another brand) megagen has 5.0mm/8.5mm implant (but the top part is actually 5.3mm) and it is slightly taper. Osstem bigger size has only got 6.0mm/5mm… megagen 6.0mm/8.5mm implant fixture the top part is 6.3mm I’m worried it will be too big.
Or can I leave it like the way it is now. And should I use multi unit abutment to raise the impression platform or just implant level impression. And also will the patient has pain on biting if I leave it like this and issue the crown?
I would leave it alone as long as it is asymptomatic . I do have a question as I have never had the confidence to rely on a surgical guide to do surgery on my behalf. If you utilized a guide and this guide was designed to be accurate to the degree that you can utilize it through a tissue punch then how and why did the guide direct this fixture 3mm subcrestal and directly on top of the nerve. I would be more concerned about who is designing these guides and why the individual is directing a guided fixture so far subcrestal, particularly in the posterior on top of a vital structure…
I am making the assumption that you provided the information to a guide fabrication service and a technician then designed your guide. My understanding is that they do this and then have the doctor ordering the guide approve the design prior to fabrication and shipment. If this is anything like the typical dental lab scenario then perhaps auxiliary personnel are doing the sending and approving without bothering you and you are left with a piece of plastic to jockey through the procedure. If this is the result of a guided procedure then the guide is flawed but cannot be blamed because it was approved and utilized by a prescribing doctor…
it is not the problem with the surgical guide. it was accurate. but I overdrilled with 5.0 drill. I should have stopped at 4.5 drill. Because the torque was not achieved. I use torque wrench to screw the implant in. and within seconds it has screwed down to 3mm subcrestal. it was my fault to drill with 5.0 drill for a 5.0mm fixture. there is no symptom now. i placed a healing abutment instead of cover screw because i used tissue punch technique. so I advised pt to not bite on that side
Then perhaps using a guide through a tissue punch is the problem. Had this been flapped and placed by conventional means I seriously doubt it would have been placed so far subcrestal as the eyes would have taken over an informed the brain that it is too deep. At any rate a guide was used and the fixture is too deep and I honestly believe that the guide, by virtue of blocking your view, is part of the problem. I am not a fan of guided placement for single unit posterior cases and I am certainly not a fan of subcrestal placement of small platform fixtures so perhaps my bias is not welcome for this scenario.
I know this is a 5.0mm diameter implant but the restorative platform is still small in the 3-3.5mm range so by my definition this is a small platform fixture and it is the same platform in which a lateral incisor would originate from… Again this stems from the Zero Bone Loss Concept which is absolutely correct but it doesn’t have to be a dramatic step down to such a small platform. Simply platform switching a 4.7mm fixture down to a 4.5mm restorative platform will provide the same level of crestal bone preservation and the fixture will not need to be 3mm subcrestal. Sure you won’t see the dramatic image of bone growing over the top of part of the fixture but it will provide the same degree of preservation and allow for a much more favorable emergence profile since the restoration can originate from a more realistic starting point.
you probably could have placed a 5x10mm implant and healing cap and bury the implant and let it heal for 6 months. i dont think you needed a bigger diameter implant. but you could have used a longer implant and bury the implant even if it torque around 15Ncm. with a 10mm long implant you would be equecrestal. At the mandible cortical bone is thick equeosseous is good enough. that’s what i would have done. 3mm subcrestal won’t be easy to restore plus. possible sausization of implant. and hygiene issues perhaps.