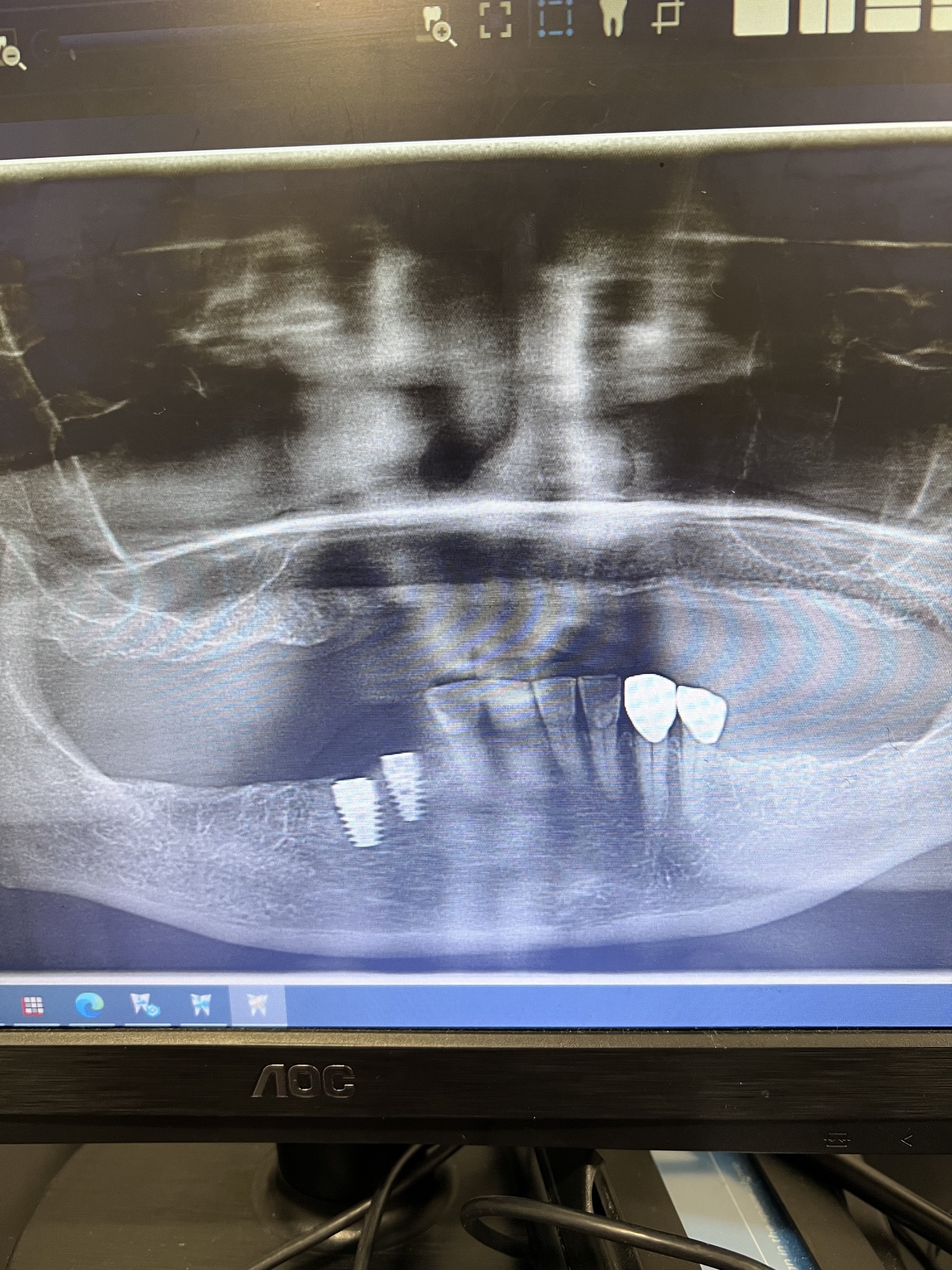
Hello!!! I am new placing implants and I am in need of some guidance, last Monday I placed two implants in position of #27 and #28, Ritter brand, during the placement I encounter some issues, while I was placing the implant for 27 I noticed that the implant was translucent through the buccal plate at the apical portion so I decided to place a bone graft, also both implants were placed to close togueter and no torque value but little mobility, what should I do with this implants? should I remove them and bien graft? On top of that the patient is a heavy smoker
kudos to you for doing 2 adjacent implants.
The parallelism looks good but they might be a bit too close to each other to allow for nice crown contours to follow . I’ve had the same thing happen to me and I went ahead and removed the one that was too close. #27 could be placed a bit more mesial and closer to the natural tooth so that you won’t have to over contour the final crown . If you and your patient have a good relationship , they will understand why you want to remove one and wait and then reposition it.
1 Like
thanks for your advise.
Agree with everything that pilot_guy said. Concerning your comment “no torque but little mobility” I think that is something that might be worth investigating. While I am not one who believes that initial stability is extremely important I do find it hard to believe that fixtures with this much taper and aggressive threads would yield this outcome if proper drilling sequence is followed. This appears to be a healed ridge with relatively dense bone so it might be possible that you overprepared your osteotomies and that is where your initial stability/torque disappeared to…
2 Likes
I have too few cases, longest duration placed seven years, so my experience will not pass any significance testing. My first 50 cases were without (digital) surgical guides, after which all are with surgical guides. With surgical guides, I do flapless surgeries unless grafting might be required.
The few cases of thin buccal plates, without perforations of the buccal plate, successful integration, even after prosthesis, up to seven years. I reason the bone may thin at the buccal point but adequate at other areas.
Buccal plate perforations, I graft, and place healing abutmentments, sometimes cover screws. During impressioning, I do not raise a flap for healing abutments to check if the buccal graft took. My first fixture placement (FDI 24) was such - buccal bone graft, healing abutment, restored and still doing well after seven years.
Those I place cover screws have substantial buccal plate stripped (planned osseodensification / expansion but not successful without buccal plate fractures), some with whole buccal fixture exposed - these are floating in the cavity in the bone - but integrated.
Like Scotty mentioned, “No torque” is certainly worth investigating. Torque does not predict success for osseointegration. All my “no torque” cases integrated.
1 Like
How the implant has no torque value? Are you sure use the right drill/implant diameter?
I think it was because I use the same drill of the implant size and no a drill smaller, yesterday I placed two more implants and use the drill previous to the size of the implant and the torque value was 35 to 40
See what our new AI platform had to say about this topic: Thin Buccal Plate and Implant Placement
Just for reference when placing a ZimVie TSZ a 3.7mm diameter fixture is placed into a 2.8mm osteotomy
4.1mm fixture-3.4mm osteotomy
4.7mm fixture-3.8mm osteotomy
Sounds like you discovered the problem. I have never used the product that you mentioned but I can’t imagine that the manufacturer would recommend placing the fixture into larger osteotomies