This video is part 1 of a 2-part series which details the treatment of a hopeless maxillary anterior tooth. Part one discusses post-extraction socket healing and site development for implant placement. Part two will discuss the steps of implant placement, provisionalization, and final restoration.
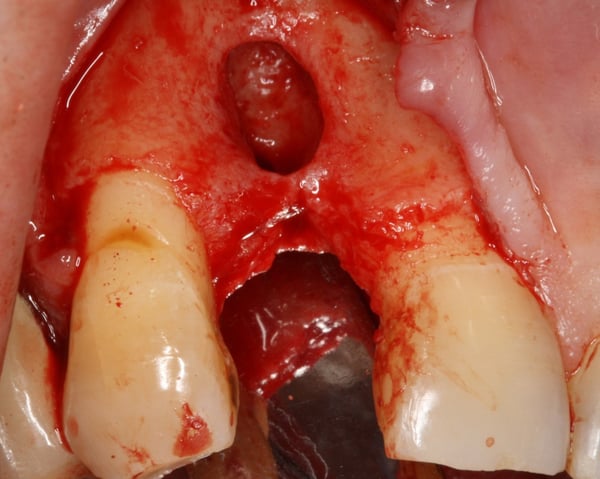
The case involved tooth 7, which had a lesion and a history of root canal therapy. The plan was to extract the tooth, and let it heal. Analysis of the extraction site 2 months after extraction revealed buccal resorption. The video explains in detail why buccal plate resorption occurs following extraction and how the defect was successfully managed in this particular case. We hope the video provides some important lessons for guided bone regeneration in these types of situations via comparison of the pre-op and post-op photos. Please stay tuned for the 2nd part of this video which will review the Implant Placement and Restoration.



robertteague comments:
Hello Daniel, Nice case and great stimulus for discussion.
My initial observations concern the graft and approach.
Approach: It was interesting to see the changes in the plate covering adjacent teeth and as you say there is no free lunch when creating the wide flap for membrane application. If a membrane is not employed the access flap can be smaller and not intefere with adjacent teeth. Such an approach reequires a form stable graft. CE markets have access to several of these, FDA markets less so.
Graft: a fully adsorbing graft will generate more de-novo bone whilst a slow resorbing one will support the volume meaning there is scope in such a case for a composite graft using both forms irrespective of origin.
Be good to watch part two when it appears.
Regards, Robert
drdangober comments:
Hi Robert. Thank you for taking the time to watch the video and comment. I agree 100% that a flap design that respects the adjacent teeth would be beneficial to minimizing facial plate remodeling. But I would not recommend doing so at the expense of proper flap handling for the GBR. It's always a fine line deciding where to place the verticals so as not to involve adjacent teeth but at the same time we don't want the flap seam over the membrane. In terms of the graft, you make a great point about the advantages of each graft type. Ideally, we would have something space maintaining and osteoinductive. If I were to do this again I would use only mineralized particulate with perhaps an outer layer of xenograft. Great discussion- hope you have a chance to watch part 2. Would enjoy hearing your feedback.
period comments:
Nice case and well presented. Would you ever perform a site augmentation together with the extraction? In some situations it may save a surgical step and speed the time to completion by two or three months.
