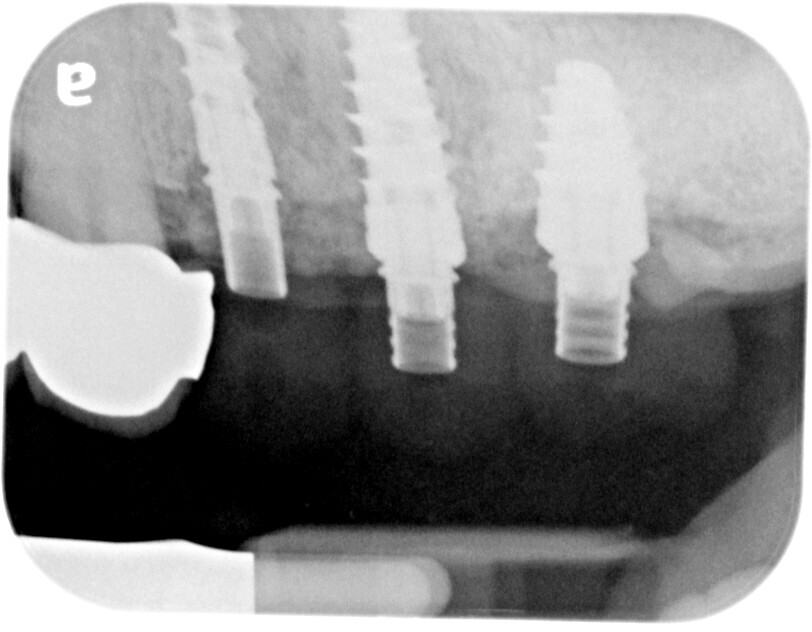
Hi, I planned to splint screw-retained crowns 12, 13, and 14 (implant sizes 3, 4,3, and 5.0 mm). Patient now wishes to have them as separated crowns for hygiene reason. I am concerned about cantilever effect on #12 and especially #14 (about 4 mm cantilevered)? What would you advise? To splint or not to splint? Another unrelated question. Would it be sufficient if I only placed implants #12 and #14 and have a bridge with #13 as a pontic? Thanks!
Randall Anonymous comments:
I never accepted the fact that all implants should or need to be splinted. I've been placing implants for 35 years at significant volume. The reason I have questioned the need for splinting was the fact that as we replace a single missing tooth with an implant we have nothing to "splint" it to. Survival rates are 95% plus.... So, why are we "supposed " to splint multiple adjacent implants.. So, NO.... I seldom splint and have an excellent 35 year survival history... Your second question....... Single implants, single crowns, always better than splinted bridge....Jeff G comments:
Better question is why do 2 of the implants already have crestal bone loss? If that is progressive then you should think about future possibilities of needing to remove one. Then splinting gives you more flexibility. Also if there is progressive bone loss the patient will have increasing interdental spaces that accumulate food and debris. Splinting probably lowers the contact points better than individual crowns.Bottom line is get a handle on crestal bone stability before restoring.
Aquiles Mas comments:
I tend to agree. I don’t splint much. If anything anymore. I believe that hygiene is super important and also managing occlusion affects things more than a small cantilever. Also trying to get a very passive fit on those three fixtures can be a long drawn out process that if not done properly can cause undue stress and possible early failure of the fixture. Also if you run into problems and everything’s splinted you are in real problems. Just my .02.Tim comments:
Don’t splint.A.Rosen comments:
Looks like the implant system you’re using is from a knockoff company … using a reputable system could save you a lot of headaches and money! Using a cheap system will always Haunt you down the roadKaz comments:
I have seen a lot of great cases done with knock off company treatment. How do you determine from this one xray that there are problems with the system. I would say that there may be a problem with the way the surgeon placed the implants. The bone levels look strange.Le comments:
Splint the 3.0 implant with 4.3 implant. It will give more strength and support to the 3.0 implant. You can have 14 be a single implant. 🔥🔥🔥🔥R Winter comments:
It is always difficult to answer questions with limited information. First, you need more x-rays and photos. Next, we need to know if there is a root tip behind 14, an overhang on the bridge at 11 or an old attachment and if the bone is great everywhere. Now for the splinting. If there is limited CHS, crown height space, splinting is advantageous. Next, if there is parafunctional habits, a history of fracture or other concerns then splinting should be considered. I would never want to give an opinion with 1 BW. Given there is periodontal bone loss on the only tooth we can see, there may be issues with that bridge/crown or other teeth. I would want to see the status of all the other teeth, the periodontal health, do an occlusal assessment and then decide the answer to your question. Also, with all do respect, why would you want to do a bridge with 2 implants if the anterior implant is only 3mm when you could and did do 3 implants to distribute force factors over 3 implants instead of 2? Best of luck and I recommend courses such as the AAID, ICOI, to give you a wider breadth of information.Greg Kammeyer, DDS, MS, comments:
I agree with Aquiles Mas. Don't splint.Richard Waghalter,DDS comments:
Hard to say if there is bone loss around the implants using a 2-D x-ray;. Might just be superimposition of buccal and lin goal from X-ray positioning. Cannot say these are knock off implants either. ./ The most important part of this case is the occlusal scheme. (Less occlusal pressure on the more anterior teeth). Does the patient has immediate cuspid rise to keep heavy forces off the posterior implants in all ranges of mandibular movement?Splintin g not necessary in my opinion. There is no indication for any cantilevers, and if there were, certainly not distal cantilevers. Overall not enough material prresented here to make definite prognostic assumptions.