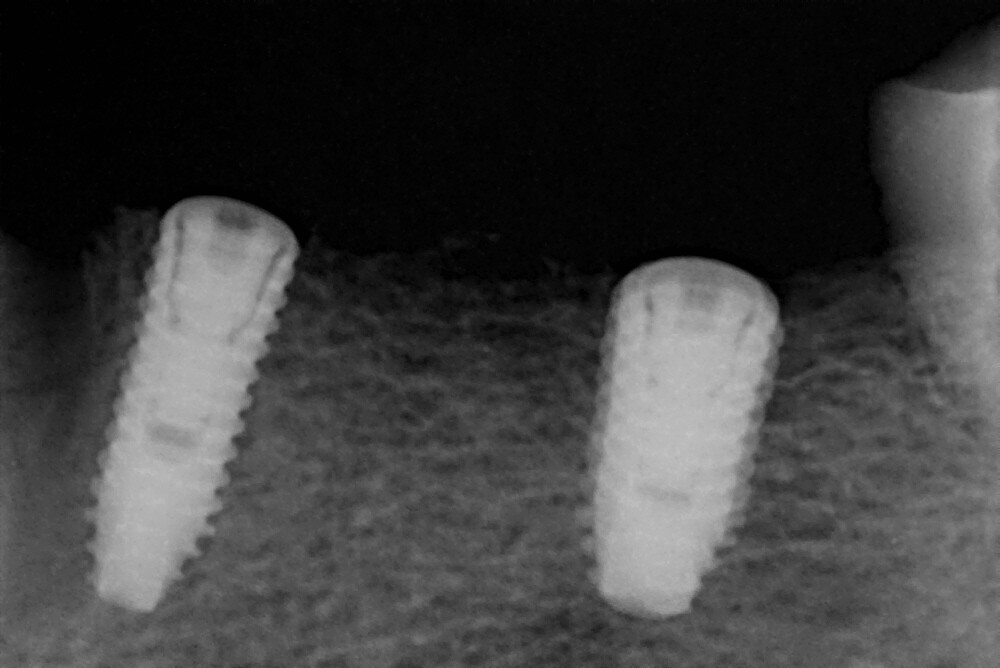
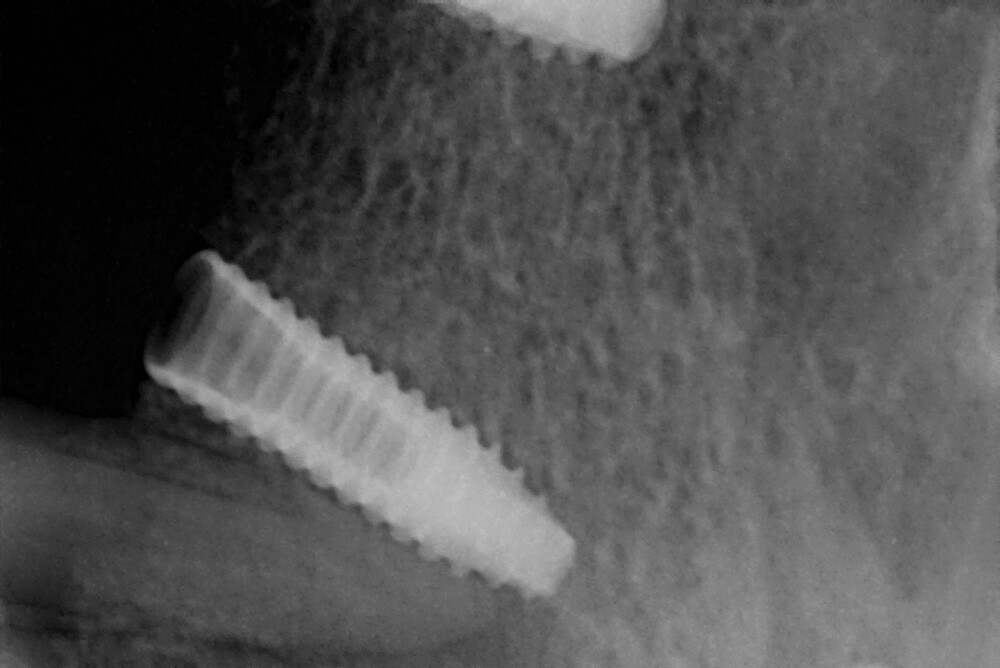
Hello. 1 week ago I have placed 2 Implants in 34 and 36 region for a 3 unit implant supported bridge wrt 34,35,36 region. But my Implants were off axis to the long axis of the ridge. RVG shows 34 implant is almost 13° and 36 Implant is almost 9 ° tilted to the long axis of the ridge. Will it create any problem during prosthesis phase? Shall I remove the 34 region implant? Please share some tips on how to place implants free hand in straight line to the ridge.
Honestly I don’t see anything wrong with your placement but from the limited data I can see on the images this patient could use a treatment plan. I don’t want to make a habit of diagnosing periodontal disease from an x-ray but at the bare minimum please remove the calculus bridge… Perhaps after you clean this patient up you will discover that a better plan might be fixtures in different locations… Seriously though its a bit early to be worried about parallel fixture placement when the patient still needs a full mouth debridement for the purpose of aiding in diagnosis.
3 Likes
Thank you Sir for you suggestion. Will do the scaling for the adjacent teeth though those teeth are mobile. This is the 10th day healing photo. Bony hard Swelling is there in the extracted 33 region which is tender on palpation, may be it is non resorb alvelolar socket ridge. And 34 region is still in process of healing. There is no pain as such, no pus discharge seen. Is the healing okay or I should worry by looking at the progress?? Kindly suggest.

Healing looks WNL but as someone who went through a 3 year periodontal residency program and has been actively involved in teaching for the past 15 years I can’t ignore the gross calculus remaining. In every teaching program that I have been involved with treating a patient’s periodontal condition is a "requirement’, not jus a suggestion, before proceeding to implant and restoration phase. Its’s not uncommon for us to be tasked with placing implants on a patient with a history of neglect but it is required of us to steer our patient’s toward better oral health prior to proceeding to the next phase of treatment. Your ability to place a screw in a patient’s bone and get that screw to integrate appears to be on par but I seriously doubt that the two implants which are the topic of this discussion would pass the litmus test of appropriate treatment. I know that patients have different wants/needs/conditions/desires/finances but skipping the first step of Treatment Planning 101 just to take credit for placing two more implants is a slap in the face to all dental professionals who follow the simple rules of common sense patient care. While your placement and surgical skills appear to be adequate I think you owe it to yourself and your future patients to consider a treatment plan before you practice drilling more holes and placing more screws. I apologize for any hurt feelings this might cause but this obvious neglect for common sense dental treatment planning must be addressed as it is beyond defense. If only bragging to our friends about how many implants we place wasn’t such a common topic of discussion among “Dental Professionals”…
Any chance this patient might be better off with an implant retained mandibular denture… Clean their teeth and develop a “Treatment Plan” and see where it takes the case…
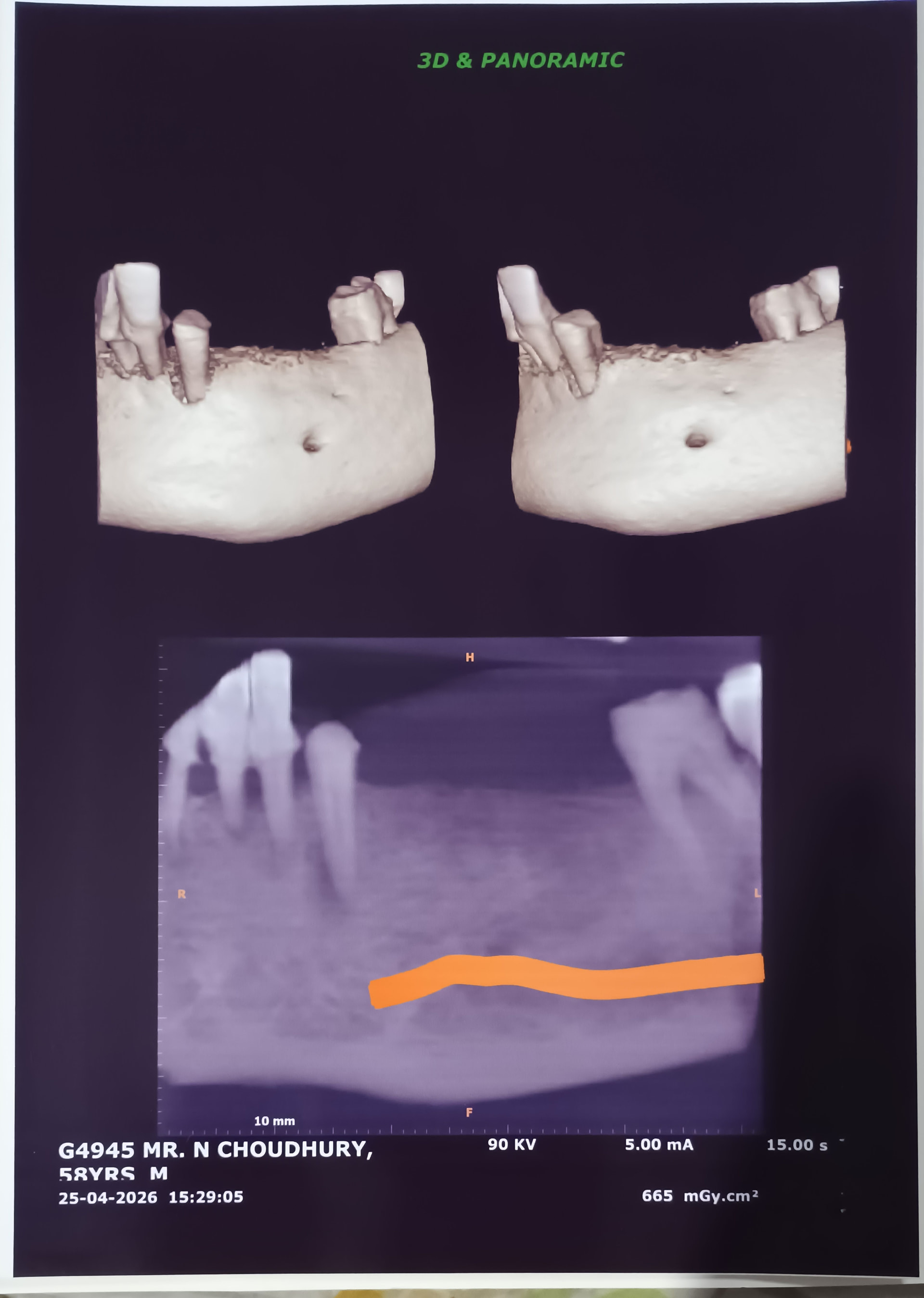
If you didn’t plan with CT and no surgical stent. There’s no way your implants will be perfectly parallel to each other. If you freehand, you need to ask your lab after you take impression. Atleast mesial distally the 2 implants look almost parallel. but the question is buccal and lingual angulation.
my tip for placing parallel implants is to place parallel pins after the first drill and take PA or PANO. and very detailly look from all directions. meaning i look from anterior, buccal, lingual and occlusal (cannot look from distal). have my assistant look at it also. when im satisfied w/ my parallelism. i’ll continue my osteotomy and place the implants. usually i can get the mesial/distal angulation very good. it’s the buccal/lingual angulation you have really scrutinize and judge critically.
but i agree with dr scotty. Please do a complete treatment plan. Your patient is definitely not a fill in the blanks implant candidate. he’s a full mouth rehab. Just because you can do an implant bridge to replace some missing teeth, doesn’t mean you should. perhaps u will convert this to an overdenture or a locator fixed in the future. but very crazy you left such huge calculus and just ignored generalized severe periodontitis. Implants are usually phase 3 of treatment planning. Other dr will severely scrutinize your treatment modality. Or are you a dr who just does whatever patient wants and if implants fail that’s the patient’s problem? Good luck.