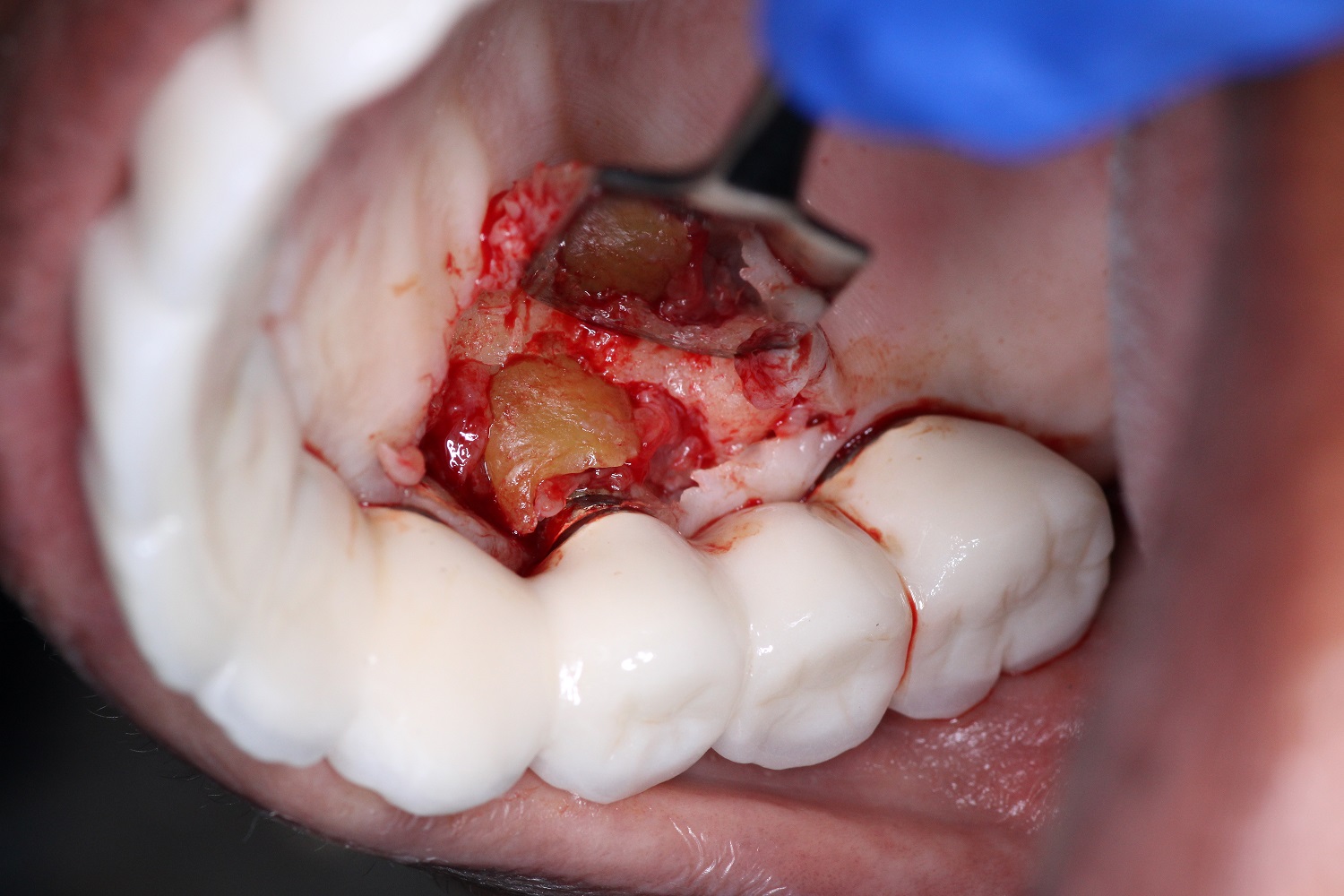
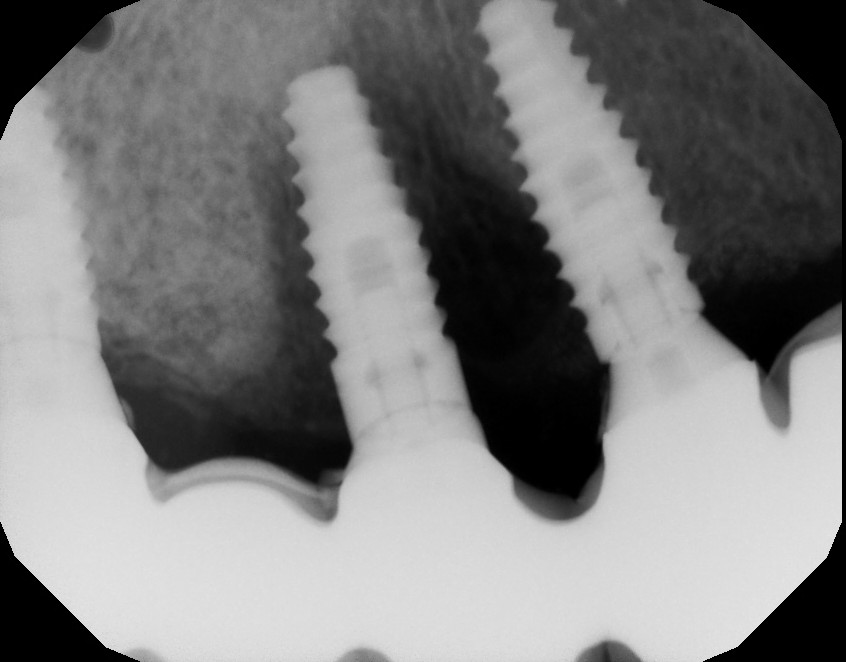
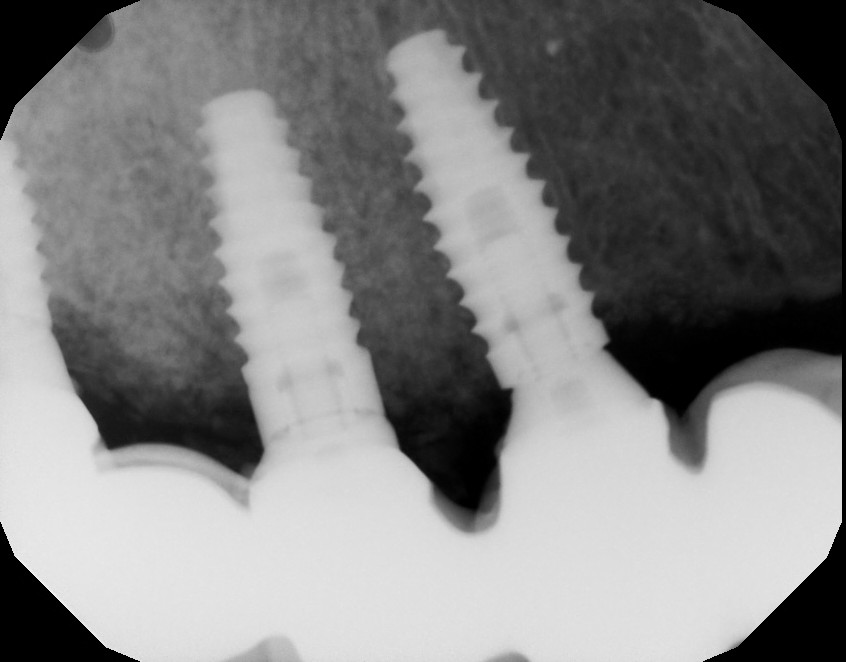
A patient presented with a chief complaint of a bad taste and pain localized to the UR posterior area of her implant-supported prosthesis which was placed a few years ago. A periapical radiograph suggested the presence of a root fragment adjacent to implant # 5.
Product Spotlight: Neomem, is the standard, sustained function, resorbable collagen membrane. It is made of Type 1 bovine collagen matrix and indicated for use in guided tissue procedures to enhance wound healing. (Neomem Sustained Collagen Membrane) Shop Now
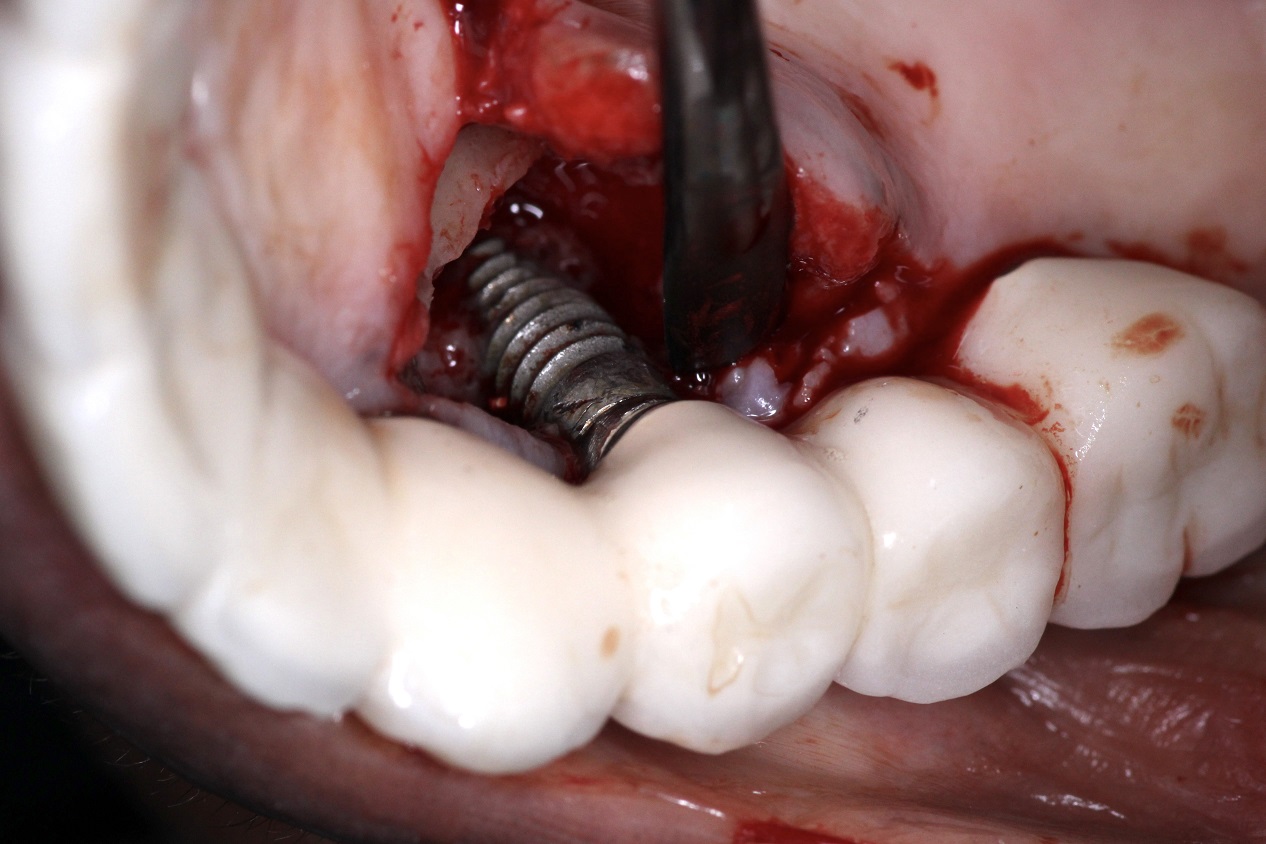
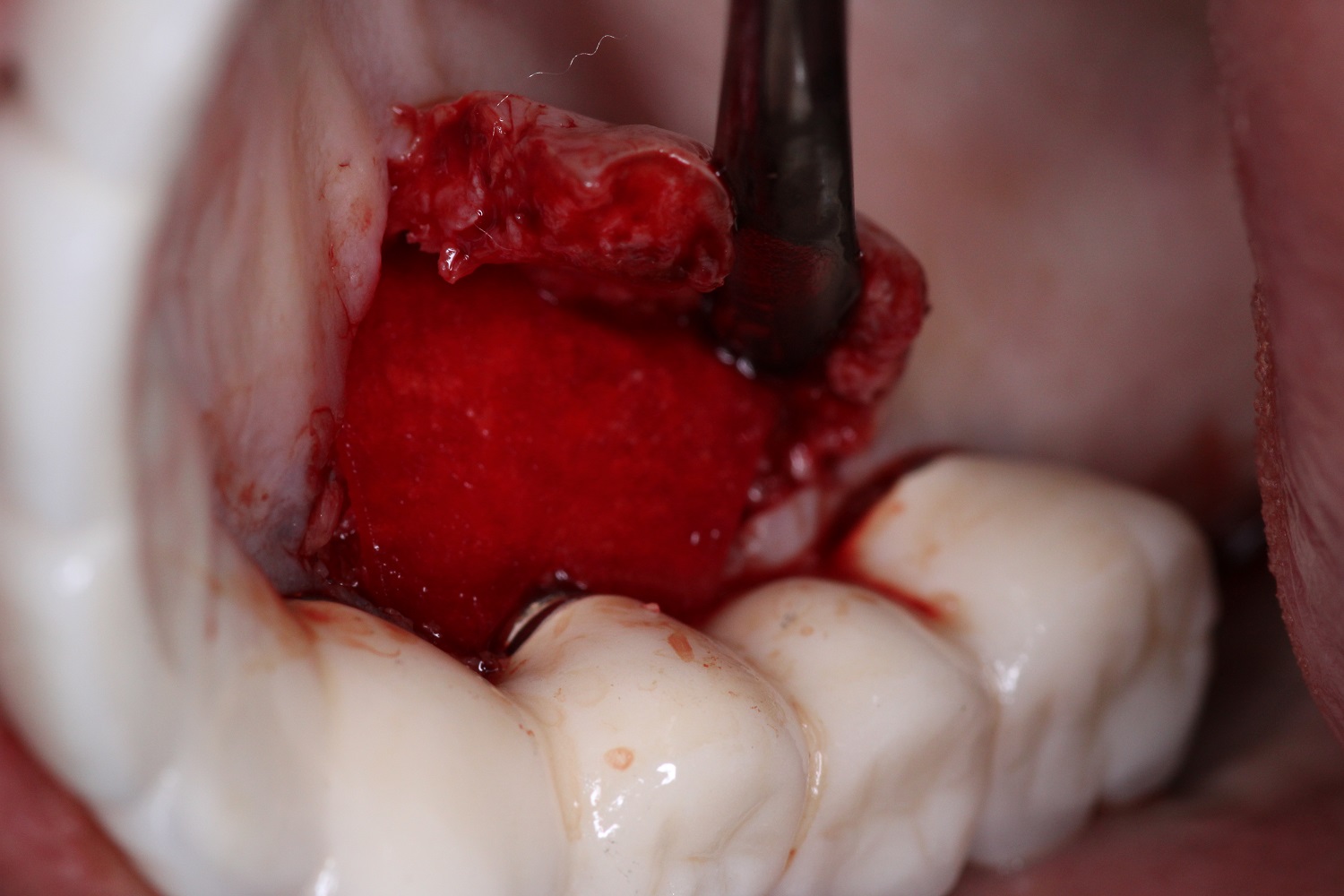
A palatal full thickness flap confirmed our suspicion. The root fragment was removed, the defect was degranulated, and the implant surface was decontaminated with a Nd:Yag laser.
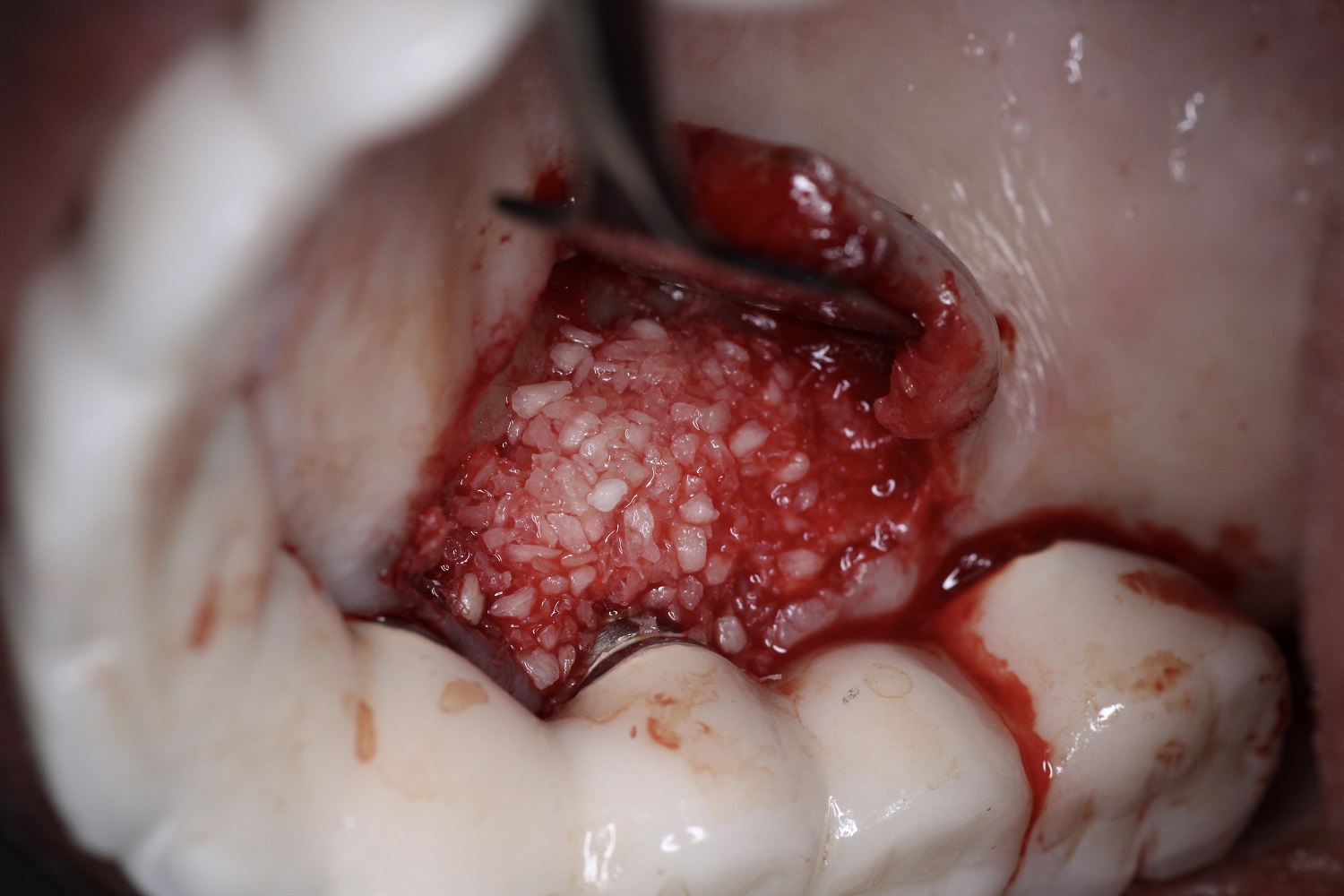
DALI cortical cancellous particulate bone was grafted within the defect and around the implant surface and a Neomem Collagen Membrane was positioned over the graft extending onto adjacent native bone. The flap was replaced with chromic gut sutures and the area will be monitored for resolution of symptoms and regeneration of the bone defect.
Great job. Something like this happened to me also. i can only assume the outside surgeon tried to do a PET on a lower 1st molar. the Dr went back to Iran while the patient was healing. Pt kept on experiencing pain and discomfort for 6 months. but that office only kept on giving pt antibiotic and run around. She came to my office. i took a PA, removed the retained roots, and grafted. Pt felt instant relief from pain after treatment. Pt end up restoring the implant with me instead of going back to the same office. Perhaps this problem is more common than i think.
Like drtoast I have my reservations about the graft actually integrating with the fixture but it should provide a great radiographic success. I don’t say this to be critical as the procedure seems to be well done and I would approach it the same way. As someone who firmly believes in grafting at the time of implant placement I do not support the concept of socket shield techniques because I believe that even an obliterated socket provides an excellent scaffold for successful grafting. If we critically analyze our work we might even convince ourselves that we can augment vertically with the help of a fresh extraction socket to provide the nutrients to a graft. Remove the root completely and the remaining socket wound will provide the ideal surface for success. I doubt that the avascular root fragment adhering to a thin avascular cortical plate is doing much besides providing the clinician an opportunity to pat themselves on the back for carrying out a published technique…
(Neomem Sustained Collagen Membrane) Shop Now