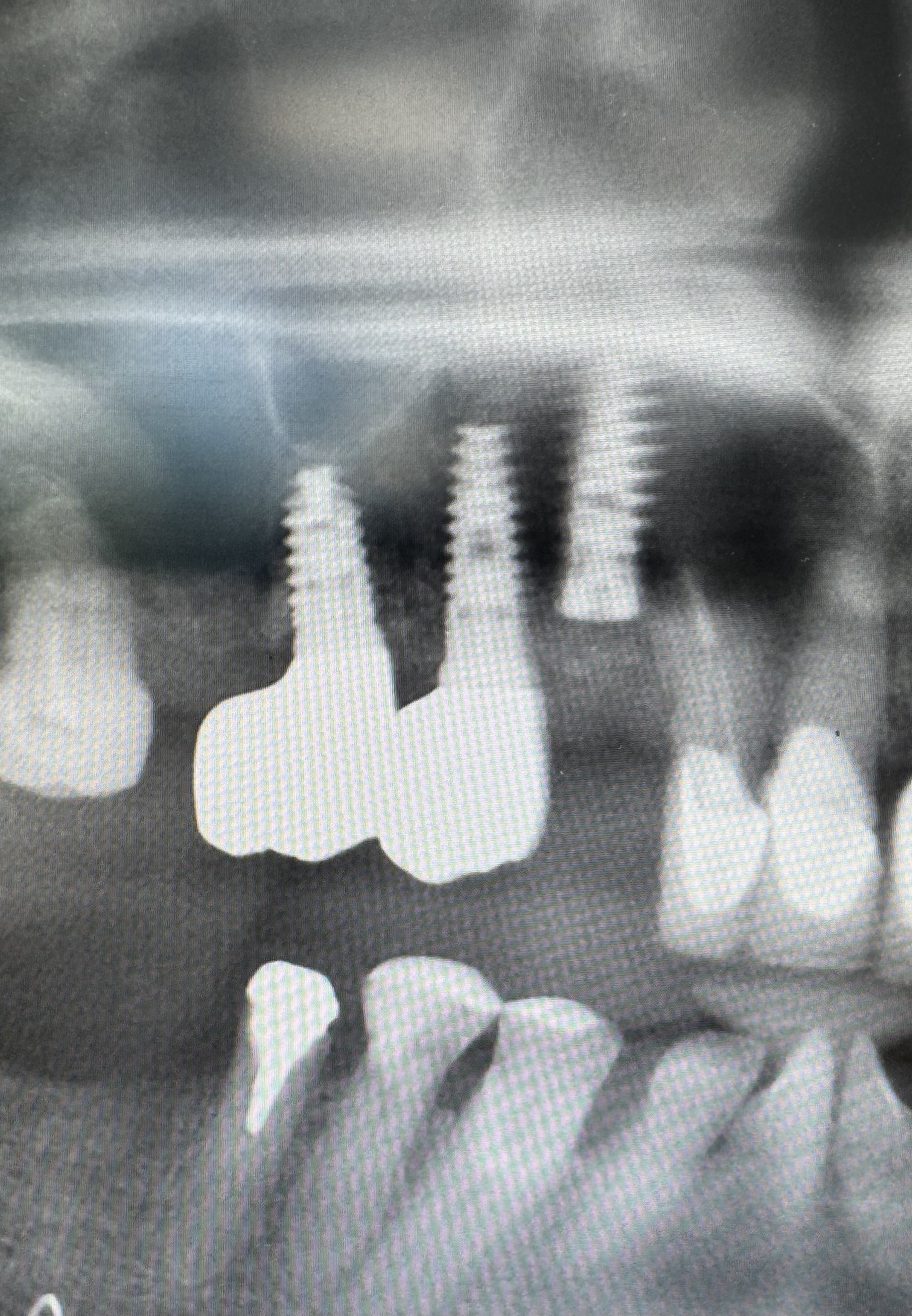
An implant 3.75/13 was placed into the right upper canine socket. The crestal bone was too narrow so the cervical part was grafted with xeno and implant pleced deeply and palataly.
The emergence profile seems to be to long now.
Would you in this situation graft the bone and place impland later on or would you just place the implant not soo deep ( only 3mm under cemento enamel border of adjecent tooth ) and so cover more of the implant body by a graft material?
Or any other ideas?
Thank you.
very difficult to ascertain implant position w/ a PANO. either you take a PA or CBCT. CBCT is best for anterior b/c you will see how much buccal bone you have. If zero buccal bone after ext. then probably delayed implant placement. but if you know how to do IDR. then you can place ext, graft, and place implant all at the same time.
the emergence profile is deteremined by the shape of your crown. not the length. there is an ideal implant position but it’s a range, you do have some room for error. your implant depth is determined by your crestal bone height. specially buccal bone height for anteriors. when implants too deep just more difficult to taken impression and restore.
I usually like to do immedicate implant. but that all depends on the aftermath of extraction and existing ridge.
hope this helps. good luck
Is this an internal hex connection?
Hi, its conical standard.
thanks, I also have a cbct. the implant was placed slightly below the level of the palatine bone of the alveolar ridge. however, the vestibular bone was missing and in this direction and also coronally the implant is covered by the augmentation. that is why it is placed so apically in the image. I do not think there should be a problem with the scan. my uncertainty concerns the length of the subgingival part of the prosthetics, which will be relatively long, i.e. the distance from the implant-abutment connection and the cervical part of the crown. I would like to know whether an implant of this type - conical standard is suitable for such a deep placement, following the example of Dr Linkevicius who works with Megagen implants.
you can place any bone level implant, doesn’t the connector type as deep as how you placed it. however, like i said, you will have trouble trying to take an impression and will be difficult to restore. Also it’s not easy to gain that buccal bone back if after extraction there is no buccal bone. I would have grafted, gain thickness then come back to place implant later.
Regarding the scan, I am sure that there will be no problem. I have a sufficiently long scanning body. The buccal bone is augmented, if healing goes well, I believe that it will be formed, however, there will also be more leverage for the implant through the length of the crown. Another thing that I would be interested in how you solve, if it occurs, is the ingrowth of connective tissue into the augmentation with a closed type of healing. If you open the wound and find that there is no quality bone near the implant after 6-8 months, should you remove it in that area and replenish the augmentation or augment the area with a CTG connective tissue graft?
If it’s a conical connection with like 15 degrees or less taper, then you should be fine. Look up what the tallest tiBase is for this connection. You should be able to get a 4mm tall ti-base. You could have a custom made healing abutment made, or you could create one yourself using a temporary cylinder. What was the insertion torque?

I have found myself in similar positions and have had to take a step back and ask myself “where is this case going”. You just placed the third consecutive adjacent implant fixture in a patient with what clearly appears to be a failing dentition. I think it is past time to be thinking about how to place and restore an implant on this patient and start considering a solution. Snap on dentures and/or full arch cases do best when implants are spread across the arch and preferably at the same depth… Multiple adjacent implants pose all sorts of problems and some of these will most likely be put to sleep if and/or when a definitive treatment plan is finalized.
1 Like
Iam not sure about the torque but it was not weak. In this case what role does the torque play?
Iam not afraid of healing process succes.
My question is how does the implant work with such a deep gingival profile?
It won’t, it will fail since it’s starting out with a >6mm Perio pocket and the lateral will fail also.