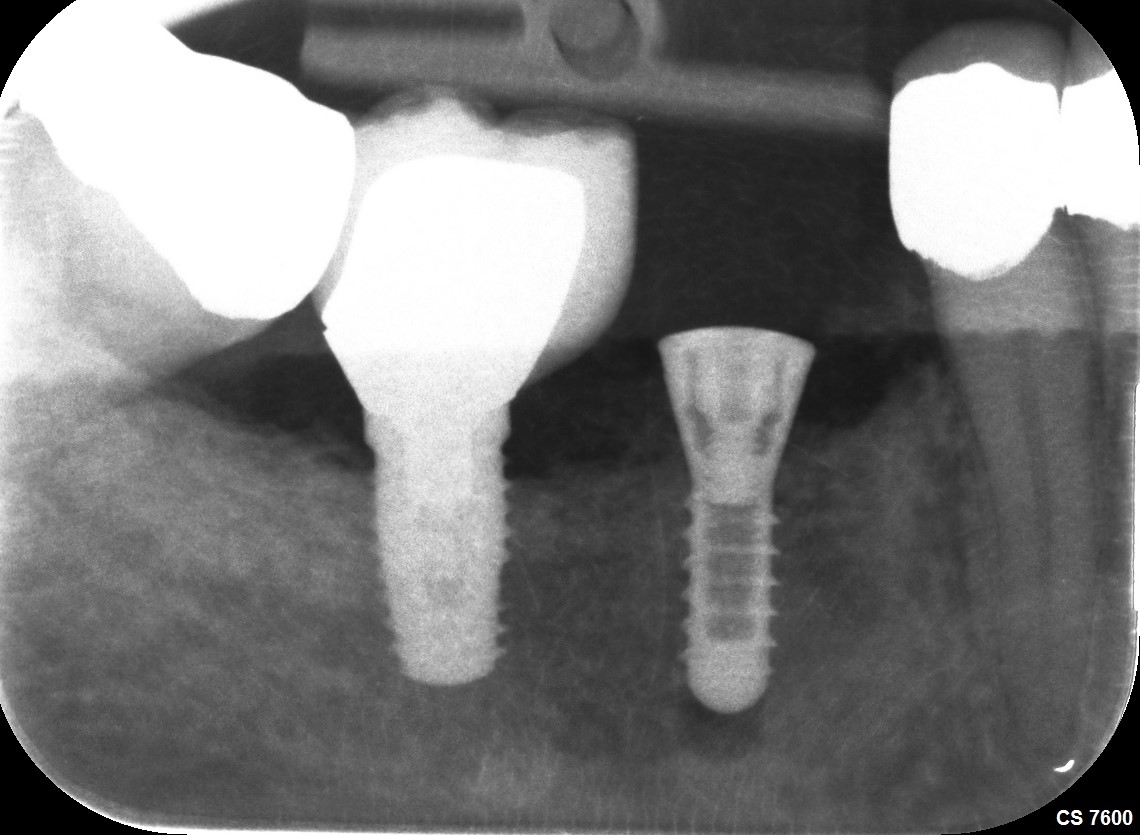
Attached is a case I just completed and it demonstrates an additional benefit of parallel walled fixtures. As can be seen on the image I intentionally overdrilled my osteotomy by an additional mm. I do this because if I just blindly drill a 10mm hole for a 10mm tissue level fixture with a 1.8mm flared polished collar I may or may not end up with the predetermined restorative margin in the proper location in relation to the gingival margin. Because of the parallel nature of both the fixture and the osteotomy I am free to seat it further apically or even back it out some to avoid a deep subgingival margin. Obviously presurgical measurements are taken but in many situations I find it necessary to fine tune the final depth of the collar. While tapered fixtures will generally achieve a higher initial insertion torque, which I have not found to translate to more successful outcomes, they do not lend themselves to fine tuning within the final osteotomy like the straight walled fixture do.
1 Like
looks great dr. you are such a proponent of parallel implants. lol
I am willing to share my experience and learning curve with others. I have placed way more tapered bone level fixtures over the years but have come to realize the beauty of this simple old school design and I intend to lean on it for the remainder of my career. I can assure you that it is not because I haven’t tried other stuff but because I have tried other stuff and the experiment has led me back to the basics.
I actually placed that 3i fixture in the #30 position 17 years ago…