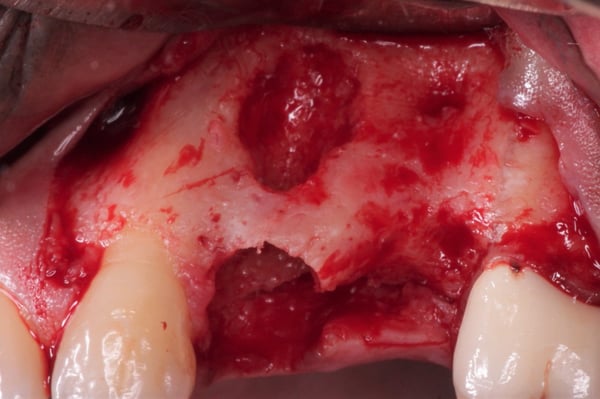
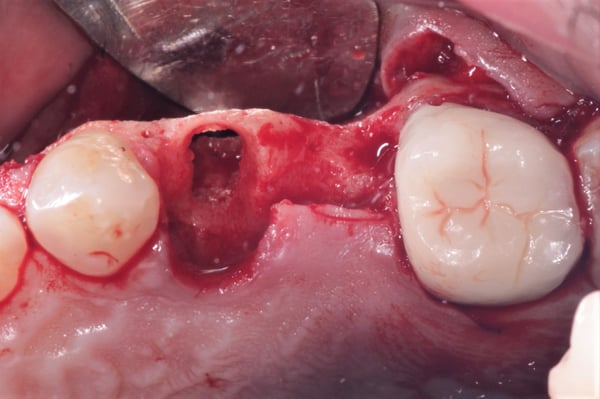
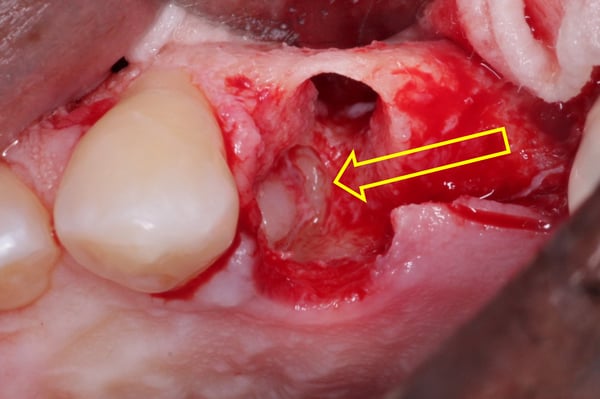
The initial radiographic presentation suggested the odontoma was not going to be encountered when extracting #12. Following extraction and degranulation, it was identified on the mesio-palatal wall of the socket. The plan is to replace #12 and 13 with implants (immediate or delayed). How would you proceed at this point?


timcarter comments:
I still do immediate... My felling is that every time a surgical procedure is performed there is a chance of adverse outcomes and the most common is recession/bone loss/dimensional since each time a flap is raised there is a degree of loss. In this case there is plenty of healthy bone to stabilize a fixture and I would lose a grand total of zero minutes sleep over that fenestration on the distal of the canine. Oddly enough I would probably opt to place the 2x fixtures, graft without the use of a membrane because everything will be contained.
timcarter comments:
Correction.. that is the odontoma rather than the distal canine but I still proceed the same way!!!
drdangober comments:
I tend to approach these cases like you. I should be seeing the final result of this case in a couple of months so would like to post it then to see what the group thinks. I appreciate your input!
ajaykashi comments:
I second that with @timcarter. You should still be able to place an immediate implant and get a predictable result.
shochfelder comments:
I would suggest nice long 10 or 12 mm implant in site #13 ( or longest possible staying 2mm from floor of sinus if an issue) and cantilever #12 off of implant in #13. Just did a case like this last week ( at least restored)
drdangober comments:
Why would you go for a cantilever in this case? Not sure I see your reasoning.
shochfelder comments:
Thank you for question. IF in fact odontoma precludes implant placement isn site 12 a single implant in site #13 with 12 cantilevered off would restore space adequately. If you like i can show you a case i finished last week with essentially the exact scenario as this with implant sites reversed ( implant site 12 and cantilever site #13. Saved patient a bit over $3000 ( cost of implant and custom abutment)
randollerton comments:
I would digitally designed the case for ideal implant position and made a surgical guide. After removing #12 and the odontoma(s) I would use the surgical guide and under prepared the diameter to length for #12. I would then use a material like Bond Apitite, mixed and placed into the #12 site and quickly place implant #12 to depth. More Bond Apitite would be placed to thicken the buccal of 12 and 13. I would avoid needing primary closure by using a PTFE membrane (TXT200) , cut to size, on site 12 tucking the B and L extent of membrane 3-4 mm's beyond the B and L bone crests. A simple Criss Cross suture to help keep the membrane in place and a little suture glue added. 4 weeks later remove the membrane. There will be new keratinized gingiva closing the socket. Uncover at a later date.
drdangober comments:
Thanks for your detailed proposed approach. When you mention digitally designing the case for a surgical guide, is this something you choose to do for all of your implant cases or were you suggesting it particular to this case?
randollerton comments:
I do it for all my cases. I'm fortunate to have a CB scanner in my office. With Blue Sky Bio (BSB) free software I can import model scans into the software and determine where the crown needs to be. I also have Exocad so it is easy to do a digital wax up when needed and it can be imported into BSB software. Then using BSB software I design a surgical guide. I can either print it out on my SprintRay Pro or if it is broken I can send the STL file to "Alien Milling" and they will print it out for about $60. I've been placing implants since 1992. A surgical guide helps me avoid so many complications, I use one 99% of the time.
timcarter comments:
That should yield a satisfactory result... My experience utilizing static guides has been much different and they have usually been the source of problems for me. I went so far as to purchase the YOMI robot unit only to return it after 1 month but that is what makes this fun as we all have different ways of achieving satisfactory results!!!
period comments:
Although a one step surgery is an advantage in a great number of cases, I would treat this one in two steps. Too many variables here that may influence the outcome, not necessarily whether or not the implants successfully integrate, but the degree to which excellence is achieved. I would graft the #12 socket. I can't tell from the x-rays and photos whether or not I would remove the odontoma(s). It would depend on whether or not removal could be easily carried out without undue influence on #11.
drdangober comments:
Thanks for your input. I definitely see the reason you would want to stage this. I personally opted to go ahead with the implant placement and graft accordingly. Look forward to the results in a few months.
period comments:
I'm sure it will work out and yield a good result. What did you do with the odontoma?
drdangober comments:
Thanks for asking. Was a tricky one but was able to fish it out.

