This 40-year old female had implants placed by another surgeon 6 months ago. She would like you to surgically uncover the implants and restore them. But, with lack of space, what do you tell her? What are her options? Please share how you would manage this situation.




smiledr comments:
This is a very tough scenario. My first thought was that the surgeon shouldn't have placed the implants. But looking at it overall, the case is a full mouth reconstruction, so placing the implants gives then time to heal while the bite is being rebuilt. Hopefully, this all was explained to the patient preop by the restorative dentist. I would open the bite slowly with an orthotic first, until stable, then prep teeth and implants at the same time. Good luck.
timcarter comments:
I am curious as to how you came to such a conclusion from the limited amount of information of two PA's and two MI photos???
kgprosth comments:
smiledr came to that conclusion based on the photographs with the limited restored of space. Therefore it needs to be changed orthodontically or with a full reconstruction in one arch to accommodate for the lack of restorative space…the VDO needs to be changed for prosthetic convenance.
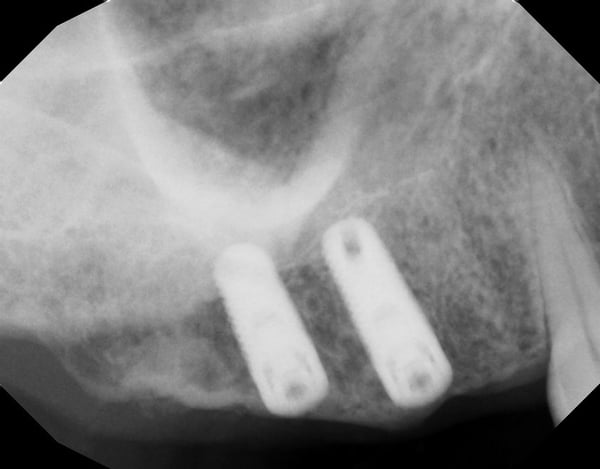
Additionally the implants on the right hand side are not prosthetically driven and will lead to a large cantilever. The implants on the left have more restorative space it appears.
One solution you aren’t changing VDO would be to remove those implants on the right followed by osteoplasty and then implants place in the proper position.
With a UCLA castable abutment you can get away with 5 to 6 mm of restorative space.
Hope this helps. KG
timcarter comments:
Without any reference for an accurate measurement I am going to assume there is about 3mm from the mandibular occlusal plane to the edentulous ridge on the right. Based on my experience having been a practicing periodontist for the past 20 years I will assume about 3mm of dense CT covering the implants leaving approximately 6mm of space. I think someone of your skill set can easily restore this case. I think a good image would be a bitewing to illustrate the actual potential restorative space... this is just my opinion based on years of working with compromised situations.
1 Like
timcarter comments:
When I was in the Army we had to present every implant case at an implant board where we used stone models, photos, and 2D plain fil radiographs as our only presentation material. I can't tell you how many times we either denied or severely complicated a case because of the perceived lack of space visible on photos and stone models of the teeth and tissue. Most of the time when the tissue was removed space magically appeared and the cases became much more manageable and I suspect that is at least a possibility here
timcarter comments:
My first thought is that the photo is deceiving because the patient has exostosis and a wide band of KG which usually translates into thick connective tissue so perhaps the thick soft tissue is masking some of the actual space. Also if you look at the left side radiograph you can see that the fixtures are placed around the same level as the adjacent CEJ of relatively normal size teeth so I would not read too much into the photo. It will be a challenge but I am relatively confident that there is more space than what initially appears from the photos.
drdangober comments:
i should have included an occlusal photo showing one of the cover screws visible. I will do so now. Thank you for pointing that out. I think that even with the CT height this is not properly restorable the way it is.
timcarter comments:
Please understand that I am not arguing with the fact that this patient has limited restorative space. That occlusal photo appears to be taken fairly soon after the procedure as incision lines are still apparent and it is clear that primary closure was not achieved over the cover screw and the tissue seems to have died back over the avascular cover screw. This patient may very well need ortho and/or full mouth reconstruction but the information provided is, IMHO, insufficient to make such predictions. I think it is likely a case of limited, though restorable space, and thick fibrous connective tissue over the right tuberosity area. I agree that the implants were not prosthetically planned and there will be a cantilever but I still believe it is a workable situation. The fixture in #3 is clearly placed more apical then #4 but the photo tells a different story likely because of the thick fibrous CT over the ridge.
drdangober comments:
I understand your point and perhaps it is worth uncovering the implants first to see what the precise space is before deciding what to do. Thank you for that POV. My original intention was to highlight the lack of planning or missed restorative dimension in the surgical phase- something we are all prone to and need to be wary of. But you make a good point in terms of the practicality of this case.
As a side point, just in terms of accurate history, the occlusal photo was taken at the same time as the others- well over 6 months since the implant placement. I appreciate your participation and input.
smiledr comments:
Interesting about the exostosis. This could be the case. My immediate reaction was based on the photos especially of the left side showing occlusion on the posterior molar. The xrays do seem to suggest that the implants on that side are submerged, even so I believe restoring the implants will be difficult without opening the bite.
smiledr comments:
Btw the original post states that there is a lack of space, which I assume is based on their clinical observation.
ninjadds1227 comments:
This is a case of poor planning and poor multi-disciplinary communication. CBCT's are required to assess. First an orthodontic consult is recommended. Next, since you don't have a 7mm (Misch Contemporary Implant Dentistry 3rd ed.) space, either intrusion is required or a VSSO or a plan to open VDO. A diagnostic wax-up is recommended along with these consults to formulate a plan. You cannot say that removal of tissue will give requisite space without measurements and this may be a case where implant removal and ostectomy will give the CHS crown height space required to perform a posterior restoration without need for more complex care.
mccavity comments:
Totally agree yet from the limited history supplied I assume there is a limited budget available to improve a life long historical dental mess. A compromise will have to do depending on present monetary circumstance.
drdangober comments:
You are correct about finances. The issue I wonder about is what options can we offer the patient short of full mouth reconstruction? Thanks for your comment.
upenn-usc comments:
I saw a new patient today who had a cement retained full gold crown on a 2molar implant.. I actually had your case in mind while observing it. BW below looks like a Misch style restoration w the abutment “flare” (or a bad impression). I’ve been practicing 20+ yrs, so am familiar w FGCs and PFMs.. you really can get away w 0.5-1.0mm thickness on the occlusal. So, if you have an older lab tech, he/she could make you a PFM w porcelain only the facial.

drdangober comments:
Thank you for sharing. That's a great recommendation! I would not have thought to design it that way.
A side point: What's your plan for #19? Can't not see it :-)
upenn-usc comments:
Would be helpful to see the overbite situation on anteriors.. most likely
full upper rehab like others have stated. The lower 1st molar (L side #19?) may be a little supererupted). There is also caries between #8,9.
Curious: Would anyone out there get creative and uncover a few mm of threads, smooth them without reducing the occlusal aspect and build crowns around them, almost like using the implant itself as the lower half of the “abutment”?
gregkammeyer comments:
When crowns are too short, several other problems occur. Uncover them and see if the space appears. If not, send them back to the surgeon.
richardhughesdds comments:
This case may need to go back to the drawing board.