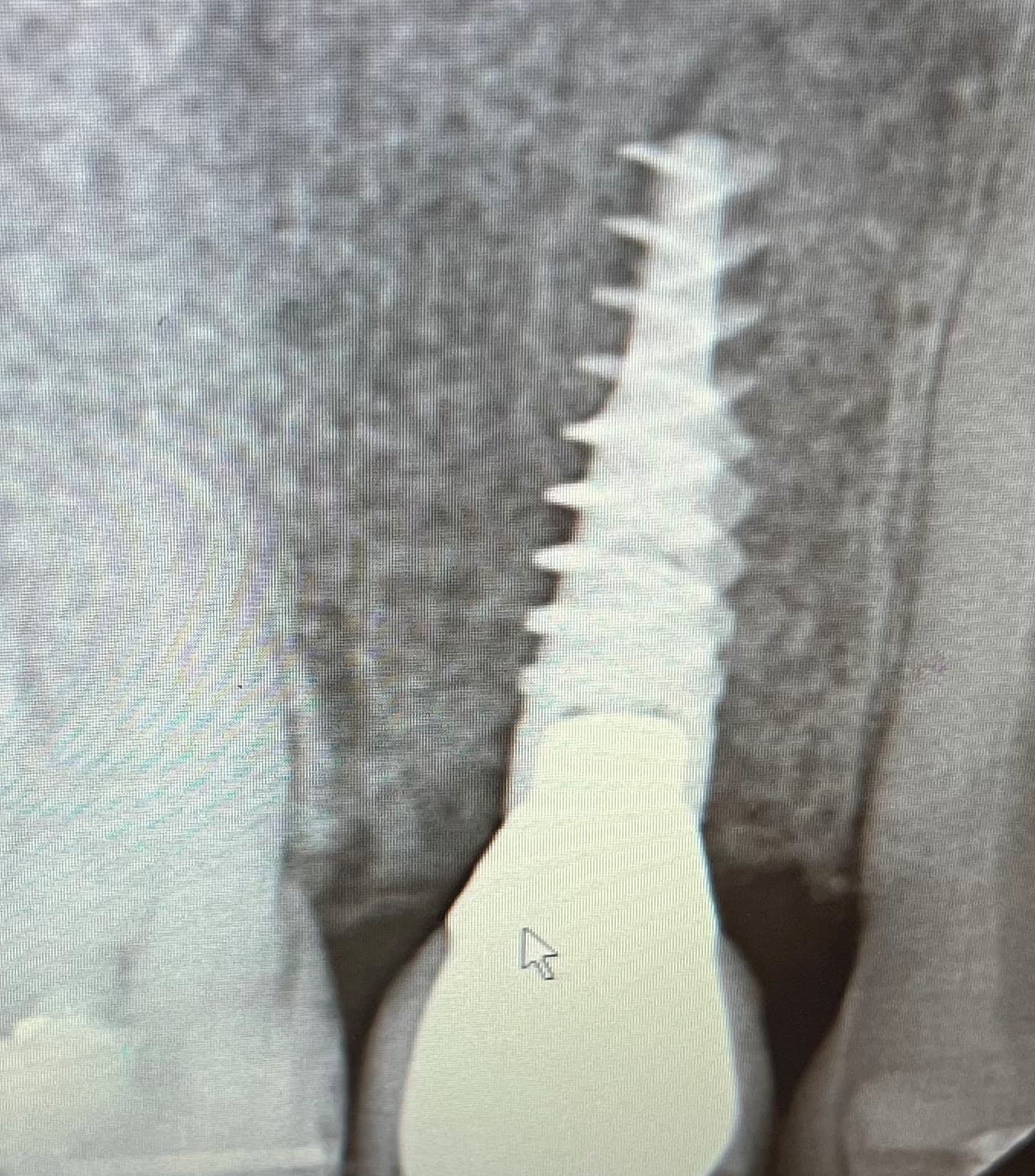
This patient was referred back to the surgeon because the implant crown had a history of loosening twice despite the dentist’s report that the screw was torqued to 35 Ncm each time. The prosthetic screw was replaced, but the crown loosened again. Once a PA was taken, it was evident that the abutment/crown was NOT fully seated which explains why the crown kept loosening. Once the crown was properly seated, the problem was fixed and has not loosened again. Have you also experienced situations like this? What else would cause a loose crown and how would you address the issue?
I would suggest:
- First: Put the crown on site… tighten to 20 Nw/cm. Put some cotton cylinders to bite strongly for 5 minutes.
- Second: repeat the rpocedure: re-tighten to 20 Nw/cm, and bite again for another 5 minutes.
- Third: NOW, you can Tighten to 35 Nw/cm… That should do, properly…
If loosen again, change the implant system.
Have a nice day, everyone
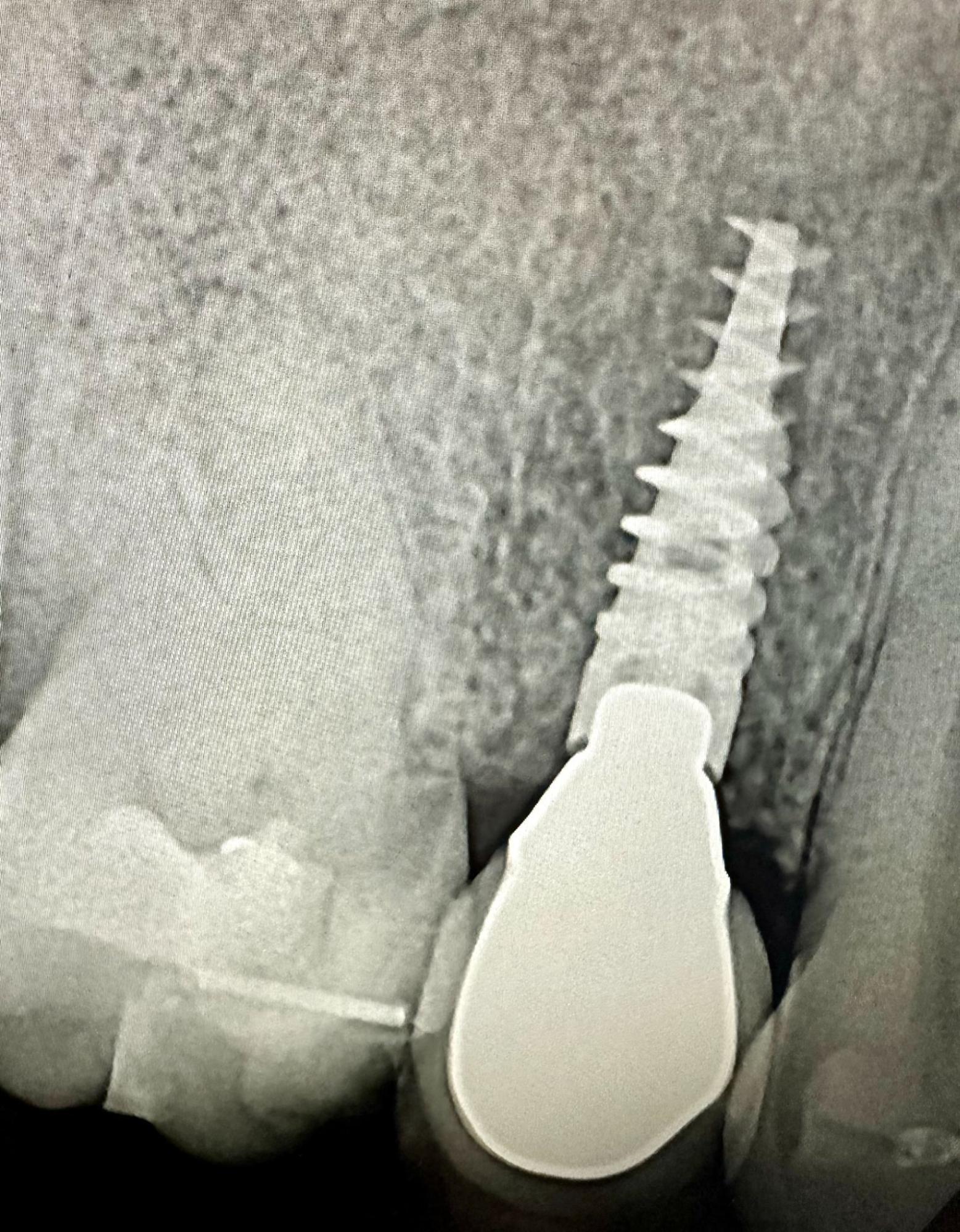
The first thing to do is to figure out why the crown didn’t seat. In this case it appears the implant was placed a few millimeters below the crest of bone and the surrounding bone could be preventing the crown from seating.
Most implants today are bone level, meaning the platform is meant to be placed at the crest of bone. When tapered implants with aggressive threading are used, as in this patient, the implant can easily get away from the operator and end up deeper than intended. Tapered implants cannot be adjusted vertically in the osteotomy which leads to situations like we see here. The easiest way to remedy this is to do some osseous recontouring around the implant platform. The Nobel system has low speed burs specifically made for this problem.
This misfit implant-abutment (I-A) connection is endemic and largely a result of the use of the screw-in installation system. The known root causes of this mechanical are 1) Dimesional Error - the difference in accracy and precision between the implant-abutment connectors and the prosthesis, when the abutment is constrained within the much less accurate and precise prosthesis. Ths abutment within the prosthesis is not allowed to realign itself with the implant during installation as it is dependent on the ability of the dentist to adjust contacts within the tolerances of the connectors.
Do you think a dentist can adjust prosthesis contacts within plus/minus 5 microns with a rotary instrument while holding it in their hand? If not - thats one root cause of misfits.
-
Incongruent Paths Of Insertion (POI). Dentists often speak of a path of insertion of a prosthesis. Implant restorations have multiple POI - determined by the implant, the abument and the adjacent teeth and other tissues. If they are incongruent by more than 5 microns you have caused an I-A misfit.
-
Resistance to Displacement by adjacent tissues. Yes, the bone and gingiva can prevent a prosthesis from seating properly.
Its hard to impossible (multiple unit installation) manage these root causes of mechanical misfit with the popular but flawed screw-in prosthesis installation system. Want to understand and prevent this problem?
Go to www.ReverseMargin.com and review my slide presentation under articles - Making Implant treatment safer.
I believe that occlusion, lack of tight, broad interproximal contacts, and too broad of an occlusal table can all or individually contribute to loosening of screws. Excursive interferences are especially effective at loosening screws. IMHO.
If that is not an aftermarket abutment then it is safe to say that this is a horrible system. I think it is fully seated just a sloppy connection. Since the implant is solid and removal is not really indicated would resort back to what my mentors did in the early 1990’s when external hex screws would loosen often. This is going to create a firestorm of criticism from all of the academic elites but I promise it works as I have done it probably 6-7 times over the years. Go to any hardware store and purchase some “Loktite” thread adhesive. This is the same stuff auto mechanics use to keep components from vibrating loose. Coat the threads of the abutment screw and torque into place. I promise it wont leach through and harm the patient and is is likely less toxic than the etch and bonding agents you use every day.
Thanks to everyone for their input and comments. It is valuable to hear everyone’s perspectives based on their experiences.
In this particular situation, after investigating this further, the dentist reported that after the healing abutment was taken off there was a delay of 5-7 minutes before the crown was placed . This may have allowed the soft tissue to collapse and interfere with the seating. Additionally, the dentist did not take an immediate post-op radiograph confirming complete seating of the crown. Based on this, it was recommended to numb the patient, remove the crown, use an instrument to push the tissue out of the way and seat the healing abutment for 10 minutes. Then try reseating the crown with no time delay. Fortunately, the crown was able to be seated completely and the crown has not loosened since!