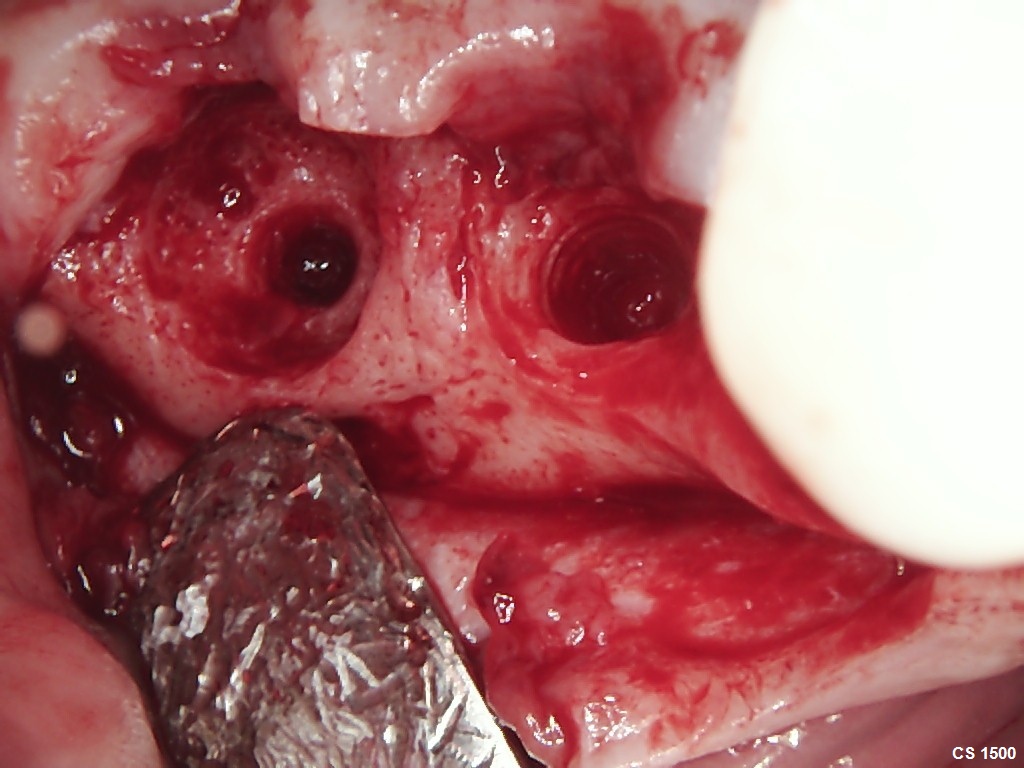
I have fortunately/unfortunately been doing this long enough that I get to see some of my past mistakes from 15+ years ago. I placed the implants back in 2008 while I was on Active Duty and they were later restored. Clearly we didn’t appreciate the importance of well contoured abutments and the Nobel Biocare Tri-Lobe was not the best at preserving that crestal bone so here is the failure after 16 years and a good example of how not to do it…


1 Like
Thanks for sharing! Learning from mistakes is the best way to learn!
1 Like
I’m glad to hear you’ve stayed in one place 15 years. Certainly the longer a dentist follows his/her cases, the more they learn about success.
I still successfully use the Nobel Trilobe for 6mm implants. These appear to be that size. It looks like the bone density is low. When I see that, I make a point of engaging the sinus floor with the implant for improved fixation.
And then there is the ever growing list of other causes for implant failure: PPI’s, SSRI’s, smoking, diabetes, etc.
1 Like
These were both 5.0x10mm… What is it about a 6mm Tri-Lobe that you like well enough to continue to use it. I abandoned the tri-lobe years ago and was under the impression that it has been all but phased out.
come on dr scotty. don’t be so hard on yourself. This case looks so textbook. 15 years ago, i wonder why u didn’t go w/ a TL implant or at that time you converted from TL to BL. Did you end up grafting for implant redo later? one of offices i go still have left over Trilobes by previous surgeon, which im trying to finish using. also, trilobe threads are very short not as aggressive as modern implants. i still like conicals. seems to have less problems and failure than other types of connection.
Dr Scotty, i did encounter a prosthetic issue w/ TL implant. a surgeon placed a TL not deep enough at #18. so the crown (restore by someone else) is short, and porcelain fractured once. i replaced the crown with monolithic zirconia on prefab abutment. hopefully it would hold up w/ light occlusal contacts.
I was on Active Duty at the time and we had a contractual obligation to use Nobel Biocare. As far as the case that you mention with the #18 not placed deep enough… that is probably the most common error folks make when placing a TL fixture. I wish I would have use TL for this case because at the very least it would have kept us from doing such a poor abutment design as the emergence is built into the fixture. Yes I did graft and will have the patient back in 8 weeks to replace the hardware
I am glad to hear that you also feel comfortable engaging the sinus floor. This particular case was done years ago and I recall performing a sinus lift prior to implant placement but today I routinely place fixtures into, 1-2mm, the sinus for the same reason that you mentioned. I actually get a lot of referrals for maxillary molars because the referring doc is not comfortable near the sinus and patients are often relieved to discover that I don’t plan to do a sinus augmentation
Well I would have to disagree with some of you comments.
I have been placing NB Trilobe back when they were sterioss. They are a very good implant , what causes most problems is crown placment and adverse pressure of the abutment on the local soft tissue. I have a multitude of radiographs showing the implant with great bone before restoration and then 1 year after restoration with ditching.
notice the circumferential ditching around the implant. I have found this is caused by excessive pressure at the soft tissue interface with the abutment and implant. They would restore these and blanch tissue when seating the abutment and back then we were cementing them.
Pressure causes inflammation which causes bone loss. Unremoved cement creates additional problems. The older style implant had an excessive metal collar that also created issues. Design changes have helped over the years. Some people buried the polished collar, I did not. I noticed bone never attached on polished collars and created a problem.
Correct placement with better abutment and tissue contour along with having the abutment support and not displace the soft tissue leads to much better long term success. I have used NB 5 mm PMC since they have come out and rarely get that problem now. The lab must understand not to displace tissue with the abutment.
Hopefull with the ability to print our own healing abutments we can shift the paradigm.
And yes they still make the NB trilobe.
Why do you think this implants received Peri-implantitis?
Good question but I suspect it has a lot to do with the poor abutment design, which I am guilty of allowing. I also believe that if we stay in one place long enough and follow our cases that we will discover the unfortunate fact that implants are only as permanent as the permanent teeth that they are replacing… In other words teeth get periodontal disease all the time and metal screws get it at least as frequently.