Hello,
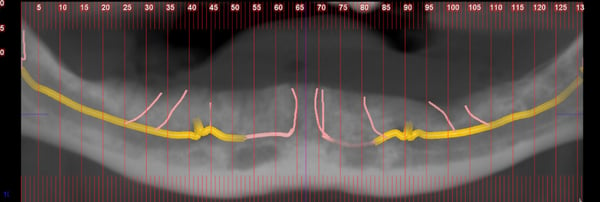
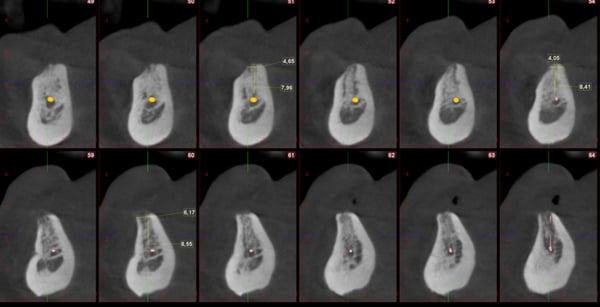
I want to place 4 implants at position LR3,2 LL2,3. See X rays attached. My concern is the possible involvement of branches of the incisive nerve which run in a vertical direction to the anterior mandible and the incisive canal itself. Do you think it is prudent to place the implants invading the lateral branches and the main branch of the incisive canal? What would be the consequences of invading the canal?
Thank you.
timcarter comments:
I find it rather impressive that you would be so observant as to inquire about such a potential complication. My experience has demonstrated that you should have nothing to worry about except I am not sure what you are trying to accomplish by squeezing 4 fixtures in such a tight space (LR3,2 LL2,3). My understanding is that the standard of care is and has been for the past 15 years or so is 2 fixtures in the anterior mandible to retain a complete denture. Your goal with fixtures in the anterior mandible should be strictly to retain a soft tissue supported prosthesis and there is no need, IMHO, for four fixtures.
andy-k comments:
Whether 2/4 implants on the mandible is determined by the opposing arch. Is it upper full denture/ full natural dentition?
Good panoramic X-ray cannot replace CBCT.
michaelt comments:
Upper would be all on six screw-retained.
This is not a panoramic. It’s a CBCT
timcarter comments:
Since there are case reports worthy of raising a concern then perhaps it would be best to minimize the potential for complications and place only 2 fixtures rather than 4. Regardless of the status of the upper arch there is really no need, that I am aware of, to place 4 fixtures between the mandibular canines. I am aware of protocols calling for 4 fixtures anterior to the mental foramina but I am not aware of any calling for such between the canines.
michaelt comments:
You are right. It’s my mistake. It won’t be LR3,2. I plan to place 4 implants between the mental foramens. The distal ones with 30 degrees inclination.
timcarter comments:
May I ask why you intend to angle the distal fixtures at 30 degrees? I understand that All-on-X protocols often suggest this but it is in no way mandatory for success. This case, unless you plan a significant ridge reduction, does not require tilted distal implants due to the abundance of vertical bone height. It would appear that you might be following a "cookie cutter" protocol and other options do exist...
michaelt comments:
Tilting the implants I would slightly increase the AP spread. What’s wrong with tilting the implants?
timcarter comments:
There is nothing wrong with it but it is unnecessary. In this case you will be able to easily achieve an appropriate AP spread without tilting the fixtures. By not tilting the fixtures you do not lock your patient into a specific restorative plan. I believe that 4 parallel fixtures are much more versatile and easier to convert if needed than a mixture of off angle screws placed purely for the purpose of a hybrid. I think the current All-on-X trend has started to create tunnel vision in the profession. I think base on the extremely limited amount of information that this patient has more available options than what is being discussed.
drcummings1 comments:
There are case reports in the literature describing dysesthesia and paresthesia
following implant placement into or near the incision nerve. I would try to avoid
this if possible
michaelt comments:
I am aware. That’s why I raise concerns.
bromike comments:
"branches of the incisive nerve which run in a vertical direction" - never heard.
timcarter comments:
This case along with the discussion that it has created illustrates something that has been discussed in the past. It would appear that the individual that posted this case intends to be the sole provider and thus wear the hat of both surgeon and restorative doc. I firmly believe that all of these case should be done with a 3 person team of surgeon, restorative doc, and lab technician. It is just too easy and far too common for a lone wolf to get locked into a specific protocol and having other team members can introduce some new prospective. At the end of the day the patient benefits from a team approach.
timcarter comments:
Perspective not prospective
period comments:
I haven't seen your restorative plan for the lower, perhaps I missed it. I agree 4 implants in the intra foramina region with a bar for support of a lower removable denture is a great plan. This is a very functional, comfortable prosthesis that can be removed for daily plaque control and for cleanings in the dental office. A fixed denture is harder to clean by the patient and harder to monitor and maintain professionally.
I wouldn’t worry about the terminal branches of the inferior alveolar nerve especially in this case where the vertically oriented branches can be avoided. I have never had a paresthesia in this area even when extending implants beyond the horizontal extension of this nerve. The sensory innervation of the lower lip is mainly related to the portion of the nerve(mental branch) exiting the mental foramina.
I can’t determine the AP spread from the parts of the CBCT scan posted here. However when needed, distally oriented implants in the first premolar sites can be valuable. Just ensure the bucco-lingual angulation is correct, that is not buccally oriented.