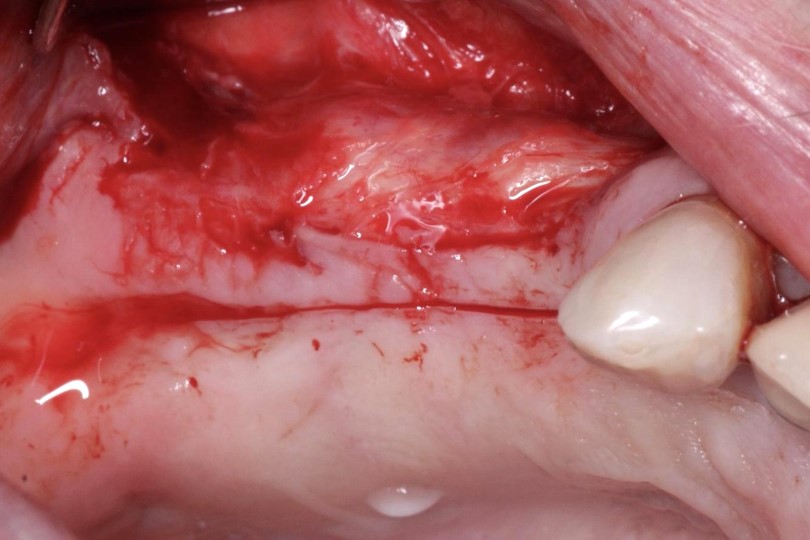
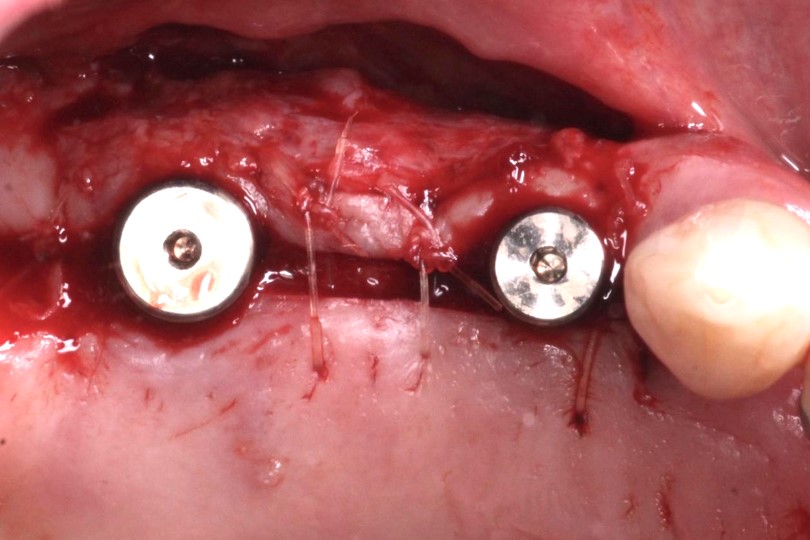
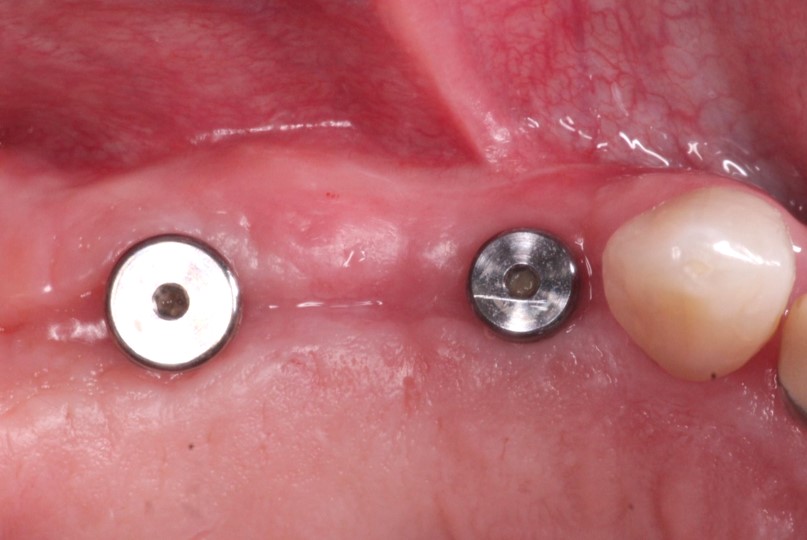
Following implant placement and GBR, it is common for the muco-gingival junction to be displaced coronally (1) as a result of achieving primary closure over the graft site. We should take advantage of the surgical uncovery appointment to re-establish vestibular depth and provide a wide zone of keratinized tissue on both sides of the implants. In this case, a partial thickness flap was used to displace the MGJ apically (2) and only then was an incision made to uncover the implants (3). The result (4) shows that proper management at the time of uncovery can establish a healthy peri implant tissue complex for the future restorations.

2 Likes
very nice. I tend to add a BioPRF over the exposed site but it looks like the site has healed quite nicely without. how was the patient comfort post op if you dont mind me asking ?
@drnewit Great point. In this case the patient did not report any particular discomfort. In general, when its a buccal/labial exposed wound I find the patients tolerate it very well. It’s typically an open palatal or lingual wound that bother them more. But PRF is certainly helpful- I happen not to use it. Thanks for the comment.
no need to suture the apically postitoned flap?
@Josh_Lee great question. Depends on how passive the flap margins are sitting. I find that in the mandible I must tack down the tissue but in the maxilla it usually sits passively enough. But if sutures are needed, then of course I suture.
Makes sense, thank you