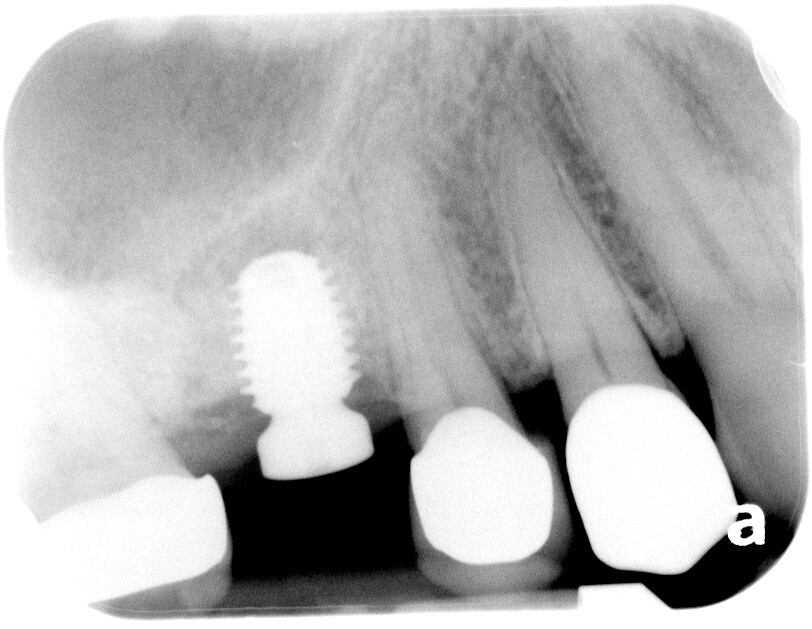
I placed this 5.0x8 implant on 5/19/23 into area of tooth #3 which has a large exotosis. Final torque was 60 N.cm and ISQ values were 82 and 82 (Penguin RFA). Today, 7/6/23, the ISQ values are measured at 81 and 83. Is this implant ready for “full-function” restoration or should I wait for at least 3 months from placement date? Thanks!
Hi. This is a great question for discussion. I think when we say wait 3 months, we are referring to the fact that in general, secondary implant stability is achieved by then with most implant surfaces. That being said, these timelines are for implants going in at lower insertion torques than yours. So in your specific case, even with a stability “dip”, it may not ever warrant waiting that amount of time to restore. Also, the implant surface characteristics and treatment will influence the rate of achieving secondary stability with osseointegration so it is helpful to know about those specific properties of the implant you are using. Personally I would feel comfortable restoring this after 10 weeks. If it were in the mandible, I would restore earlier at 8 weeks. (But I cannot claim to support this with too much scientific evidence).
Let us know what you decide to do and how it works out.
1 Like
I would trust my investment if I were you. That Penguin RFA device surely wasn’t free and I assume you purchased it for some reason relating to “when” to load an implant fixture. If these devices are worth the scrap metal and plastic to construct them with then a reading of such after 4 weeks should be a green light. I personally purchased a similar device about 8-10 years ago and used it for a very short time before resorting back to my original routine of just waiting 10-12 weeks for everything. I guess my advice would be either to trust your gear or abandon it all together because if you can’t trust it then it is just scrap metal and plastic…
1 Like
Before you send that Penguin RFA device to it final resting place in your closet I would suggest that you do some comparisons of immediate readings of implants placed with high torque values (>45Ncm) vs those with modest insertion torque (15-30Ncm). When I did this I was often times amazed at the greater ISQ readings with some of the lower insertion torque fixtures vs those placed with a cheater bar. While I can’t tell you where my RFA/ISQ device is today I can say that it changed my view on primary insertion torque as it relates to resonance frequency values and today I feel much better about a fixture placed at 30Ncm then I do one placed at 50+ so the end result is that I have been forced to use clinical judgement rather than numerical values.
1 Like
I have found that initial primary stability is an over rated metric for success. This concept was all the rage with tapered implants, and in my mind, really blown out of proportion.
You can easily achieve > 50 Ncm insertion torque with two implant threads engaged. In this case, your bone implant contact is minimal, but your ISQ is high, and this implant is at higher risk for failure then one with a lower ISQ and more bone implant contact.
ISQ readings at placement have poor correlation to implant bone contact.
I’ve had spinning implants ISQ at 85 after 16 weeks.
I place my implants at much lower insertion torques then I used to, and the results are good
Even with immediate load, full arch, etc… I don’t see the need for the kind of insertion torques that I see labeled as “good” Do I have a number that I shoot for? No- i like “solid” with a crisp high pitched click when I percuss the healing abutment.
All that being said, I ISQ check all of my implants before sending the patient to the restoring DDS.
Every once in a while, I catch one that failed to integrate.
2 Likes
Although your data suggests that this is ready to load, is waiting a couple more months really that big a deal “to be sure” it has integrated? Especially if we are talking about a restoration hopefully being in the mouth for 20-30 years?
1 Like
I agree with you and that is exactly the rational mindset that calls into question the clinical relevance of such a device as the ISQ. This is coming from someone who has an Ostell unit collecting dust for the past 7 years somewhere around this office… If you can’t trust the device, which I never could, then perhaps it should not be part of the final decision to proceed. I hate to repeat myself but it was really interesting though to see just how unimportant insertion torque is to ISQ value.
2 Likes
My ISQ machines are well used. They’ve saved my bacon, from an unhappy referral more than a few times, AND I found waiting longer than 3 months, when the ISQ was low, on many cases is all it took…esp for those folks that don’t exercise. Why not use it? For the cost of the pins, it’s money well spent.
Waiting 2-3 months isn’t a deal breaker for most patients. 3 months is a bone turnover cycle in humans and is worth the wait. Why mess up a good thing, that clearly is working?
@smiledr I guess this would depend on what one believes has occurred by 3 months. If integration has occurred, then waiting additional time is unnecessary.
Please could you guide me how to know that ossiodensifaction has taken place and implant is ready to load with out that .RFA digital device . Any clinical tips