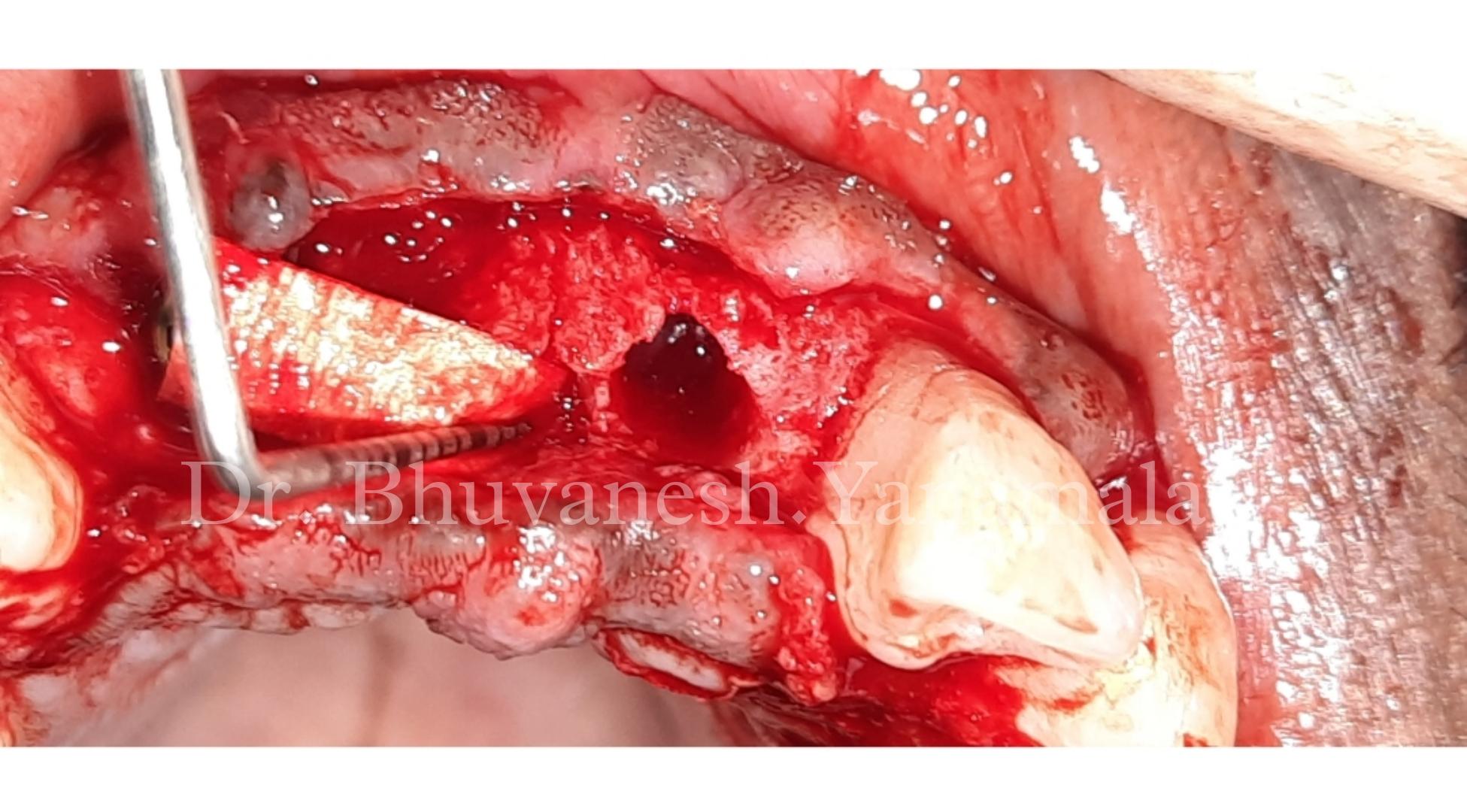
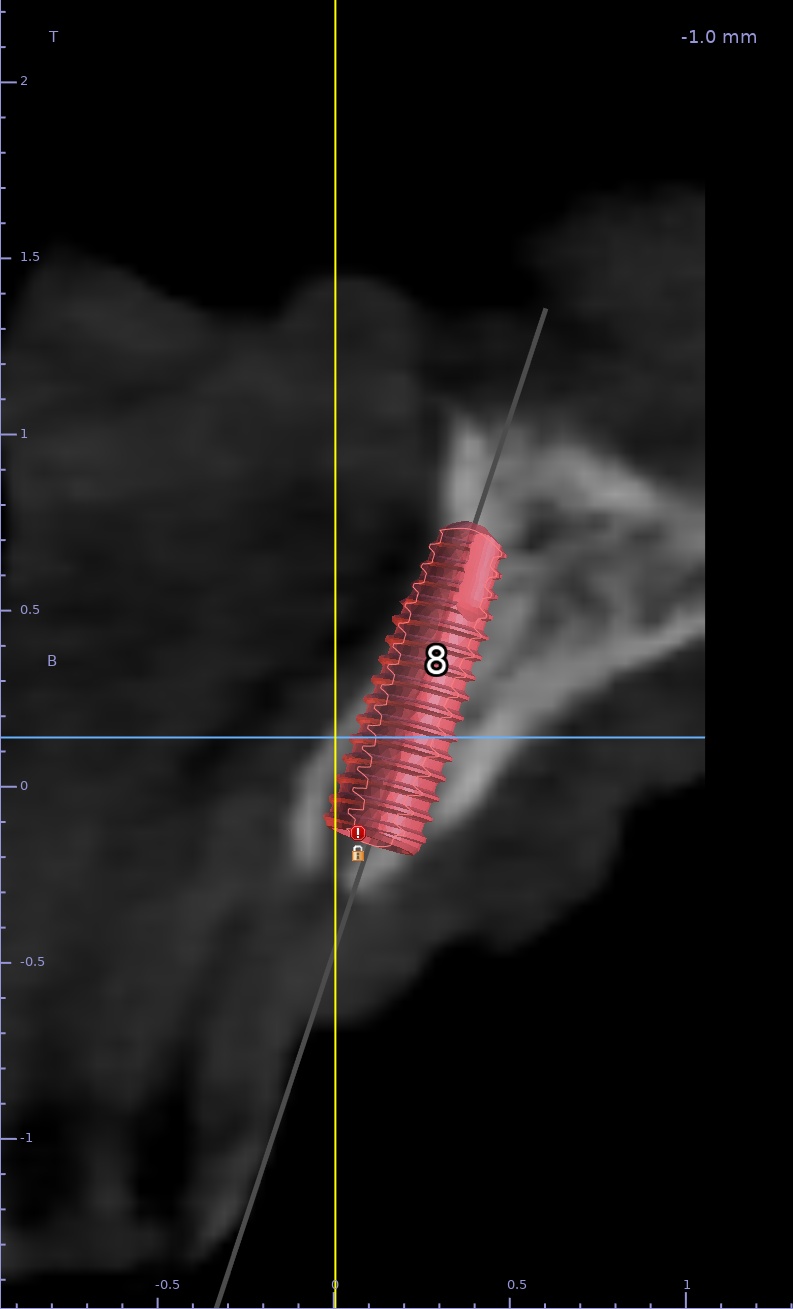
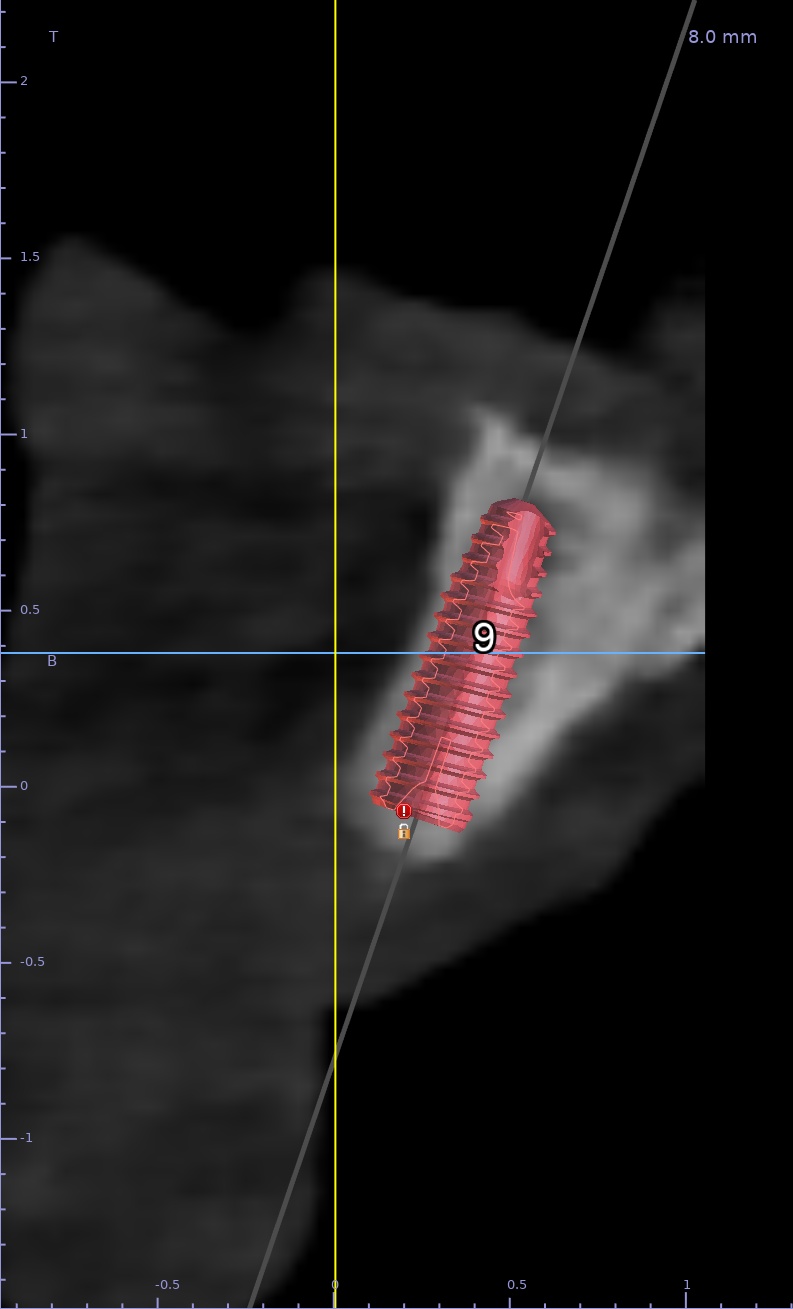
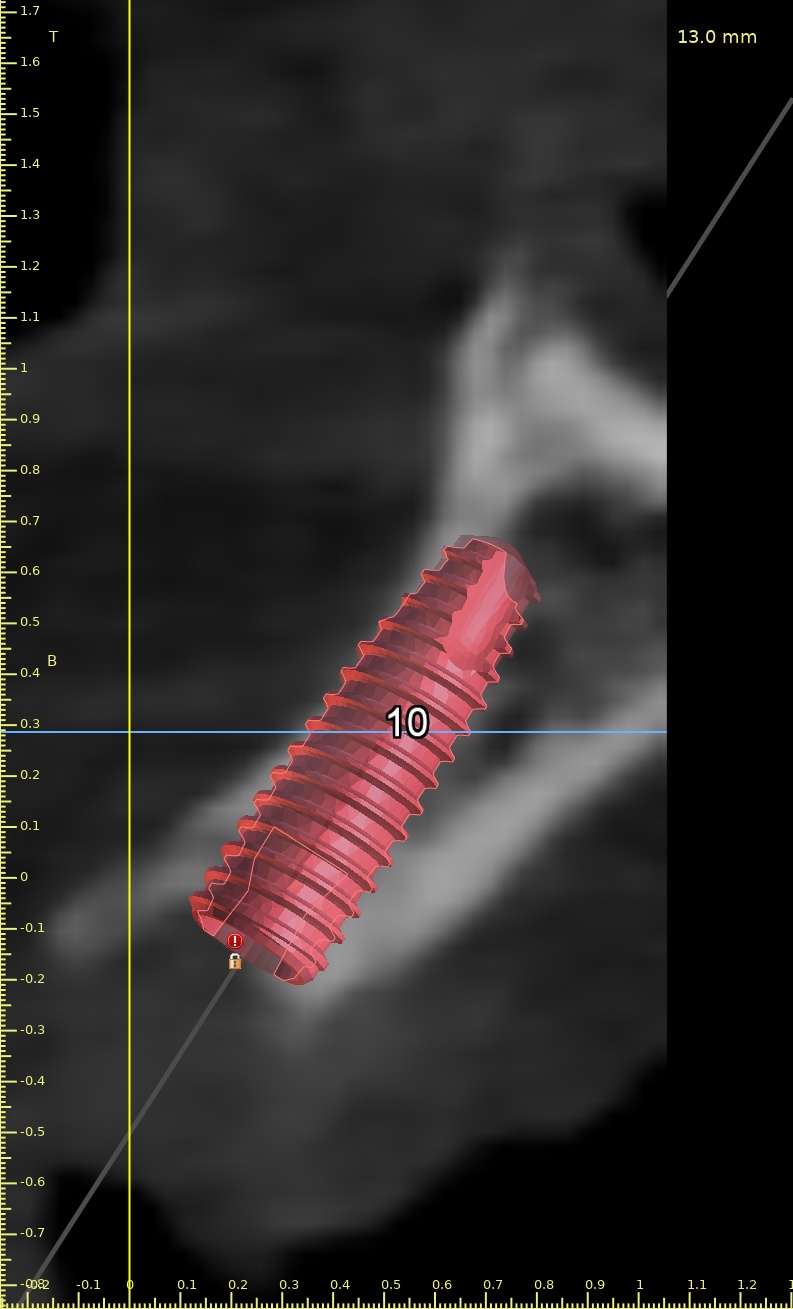
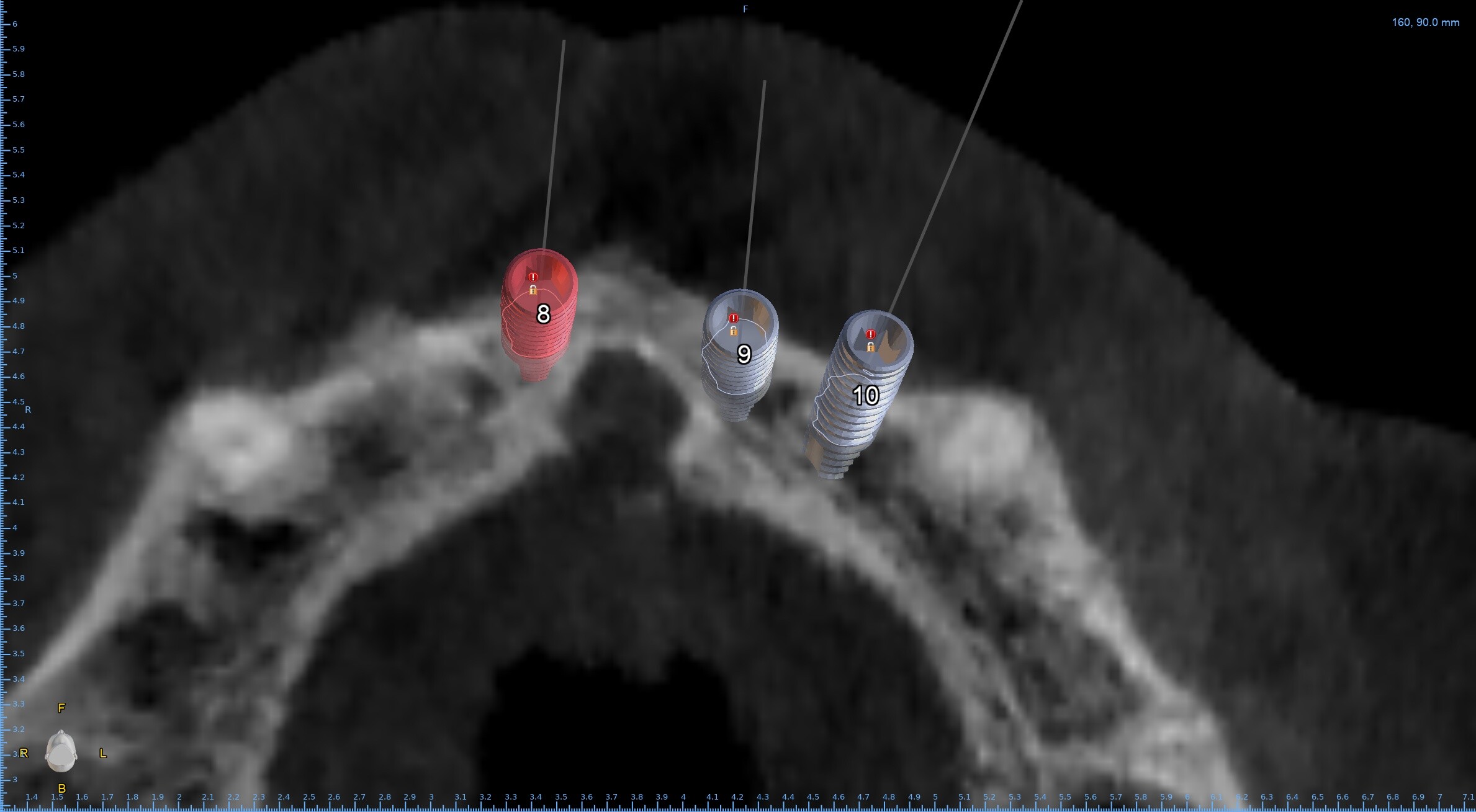
Hi, I plan to place implants for #8-9-10 bridge. The incisive canal is so large and implants #8 and 9 are very close to the canal. Any advice? What should I do if the canal is perforated during the osteotomy? Thanks!
GK comments:
The case would most likely need ridge expansion and if the osteotomy breaches into the incisive canal (which u can check visually and with a probe the integrity of your osteotomy )in which case you would need to empty the contents of this canal and possibly graft here.The patient must be adequately informed and consented for this and it's possible effects of tingling numbness etc.This is my thoughts on this case.Justin George comments:
Could you share on how you would go about and empty the contents of the incisive canal i.e what is the best way to do it ?T N comments:
Here are some info i found:

T N comments:
One more...
Cheers!
Tim comments:
The canal is of little concern as it can easily be managed just like GK described. What concerns me is why you are planning 3 individual implants 8,9,10 rather than 2. For obvious esthetic reasons I would suggest rarely, if ever, place a central and adjacent lateral. Consider managing the canal PRN and reconsider the proposed plan. Possibly implant 8-10 with a 3 unit FPD…Steven Hochfelder comments:
Tim i totally agree with your above comment and of course save $2500-3000 probably with the implant/custom abutment if 3 individual implants done vs 2. Also as mentioned implants adjacent limit to some degree esthetic options with a pontic design more flexibilty to enhance estheticsGK comments:
Hi Tim So do you mean implant at 8 and 10 and a bridge to connect these right?Tim comments:
That is correct and would be ideal. Another option would be implant 8 and 9 with 10 cantilever. Placing a central and lateral adjacent rarely produces an acceptable esthetic result and my experience has been to avoid such when possible. I would have to go back to my office and review some of my lecture slides for the exact reference but there is a great article by Salama dating back to 2007/08 ish that I often share with residentsNeil Zachs comments:
I Agee with Tim....The canal is of little concern. The bigger issue is the three implants. Definitely space for a bridge with 2 implants. The incisive nerve is the one nerve that is resilient. The other issue is your placement. WAY TOO FAR BUCCAL and too wide or the ridge. This will be an issue long term. These cases should be done FULLY CT Guided.Neil Zachs
Periodontist, Scottsdale AZ
HD comments:
Your angulation is incorrect and your gonna destroy the buccal plate but other than everything looks great . Go for it ! :grinning:Greg Kammeyer, DDS, MS comments:
It is acceptable to wipe out the incisive canal contents, and on some cases you may want to use the canal for an implant sight, Remember you need approx-2mm of buccal bone and 2 mm of soft tissue to maintain long term stability...otherwise you will get recession. Remember too that an incisive canal cyst is not unusual. So a couple of areas to study. lastly the case will be more esthetic if its a bridge on 2 implants.Bhuvanesh Yanamala comments:
We did similar case sir, using versha osseodensification burs, later by moving the contents and grafted the canal