Today i inserted imediat postextractional a Bredent copaSky 4x14, in socket 21, after a Root fracture in the middle.third.
The case was made using a radiologic surgical Guide. The extraction was perfect, without any bucal bone fracture, or trauma for the soft tissue.
The torque was poor around 25 Ncm. I tried to engaged more apically but stilul no high torque, stilll 20-25 Ncm.
I made buccal gbr with bone graft, prf, and CTG. The implant îs 5 mm bucal , drom the gingival margin, and 3 mm from.the buccal plate. I made a customed healing abutment.
Should i make.a maryland? Or reentry, remove the implant and put a megagen 4.5x13, and try to load?
Was a fully digital surgical guide used? Why did the implant appear to be placed too deep? Looking at Figure 2, the labial bone plate seems very intact. If I were performing the surgery, I would not raise a flap, but rather place bone graft material coronally in the jumping distance, compact it, and then perform a simple free gingival graft. As for the current situation, you could make a temporary denture with a transparent vacuum-formed spacer.
Could you remove the implant, place some fine small particle cancellous bone with a small syringe and then drive the implant in to a more superficial depth and get better primary stability?
Rather than remove-retraumatize why not leave it in place… I am still loyal to Zimmerr TSV which is an old school fixture design so I am not a faithful disciple of the “Zero Bone Loss” concept but this appears to be a fixture designed with this concept in mind. Given that “Zero Bone Loss” is so widely accepted and promised within the implant industry isn’t this an acceptable placement? It is only a problem if you experience circumferential bone loss around the fixture and per the manufacturers promise that will not happen here so you should be fine. Leave it and let the promise of the design handle the rest!!!
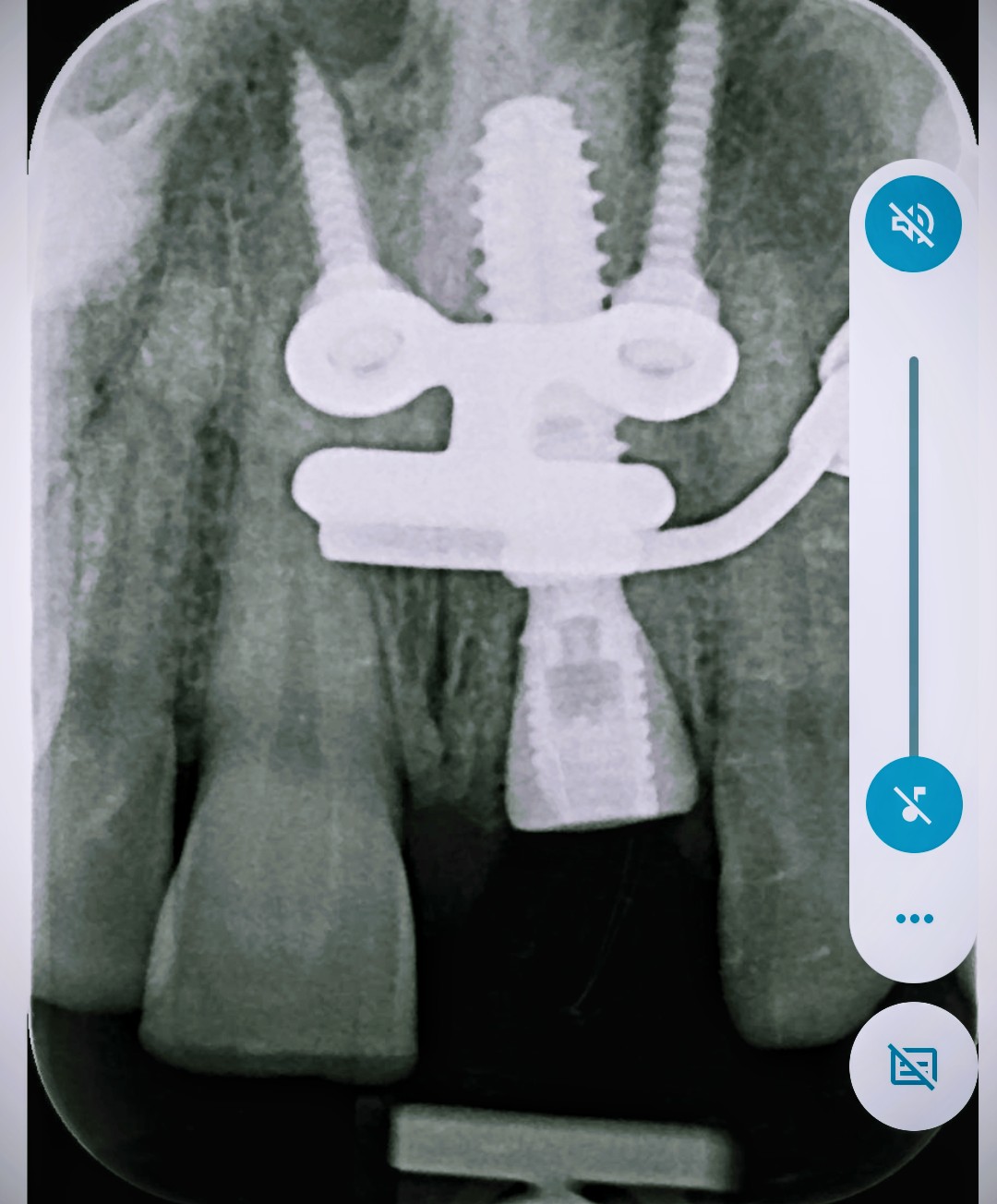
im confused. how you know your implant is 3mm from the buccal plate. the sagittal view you provided is a planned implant position not the actual CT scan of post implant placement. from your PA. the implant seems more than 5mm from the gingival margin. more like 8mm.
if your extraction is perfect. you shouldn’t need to GBR, PRF, CTG. you only need to place BG between implant and buccal plate to fill the gap which is 2-3mm at most. the custom healing abutment would preserve the papilla and no need for CTG. PRF and CTG is useless here in my opinion. definitely not neccesary.
Also what’s that screw and plate? is that the surgical guide? couldn’t you use just a tooth supported surgical guide. Kinda over kill and more trauma for single tooth site.
I would definitely not remove and redo implant. using a bigger implant is definitely not the correct answer for anterior implants. I feel like this case was made more complicated.
in my hands, just extraction, free hand immediate implant placement, BG to fill the gap if buccal plate intact and place cover screw, collagen plug and PTFE suture and let it heal. i wouldn’t even bother loading b/c my patients dont want to pay for immediate provisionalization. come back 4 months for 2nd stage. then impression and deliver crown. recently i even do impression at the time of 2nd stage. save time.