Two dentists offices i’m seeing disagree on what to do about tooth number 14, which has been inflamed and infected for a few months.
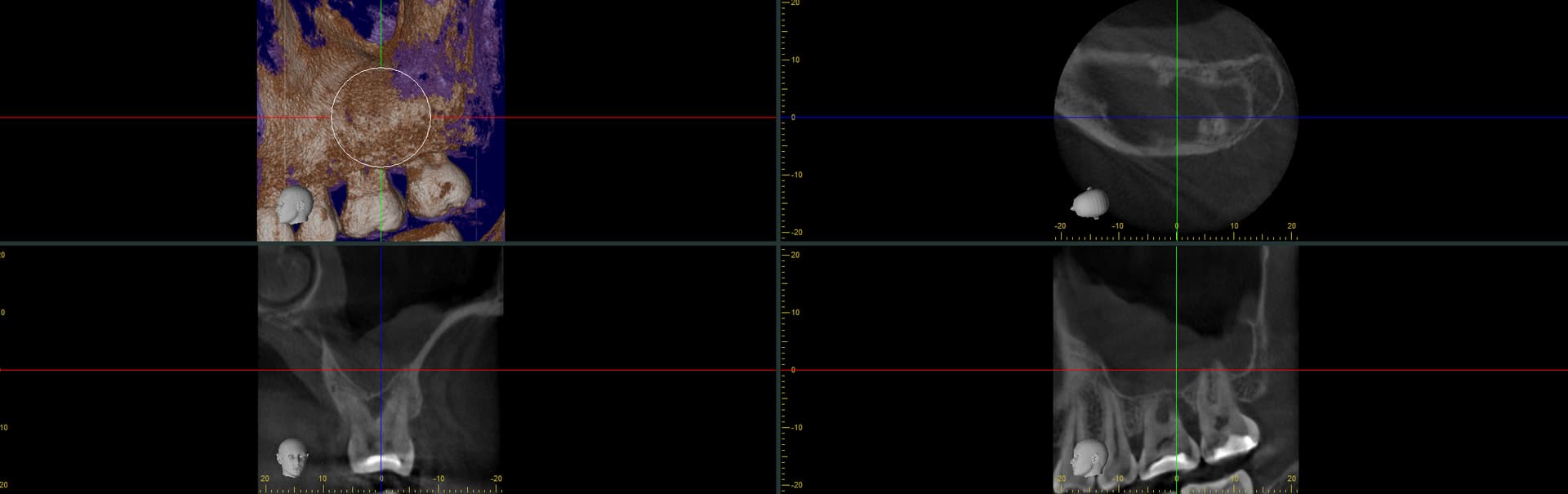
office 1 took this CBCT and believes that this is an endo-perio problem, with an abcess existing at one of the roots of number 15, as well as the obvious bone loss. Office 1, led by a periodontist (didn’t see an endodontist here) thinks that the best course of treatment is extraction and implant because trying to save the tooth by doing a root canal and perio surgery would have a poor success rate.
Office 2 believes that there is no endo problem. The endodontist here did some standard sensitivity testing and examined it, and concluded a root canal is not needed. The perio at this office wants to do an osseous + bone graft because this office believes this is a purely perio problem that can be solved without extraction given little-no mobility.
I have no idea who is right here. Is office 1 correct that there is an endo problem/abscess? Should I send office 2 the CBCT and see what they say?
i know you’re a patient. This forum is primarily for dentists to discuss our cases with colleagues. But i will try to help you. If the tooth is symptomatic, giving you problems, there are only 2 options, try to save (RCT) or ext. RCT will involve restoring the tooth including post/core/crown. CT are viewed as a whole. the 4 pics you uploaded are not completely helpful. the tooth could also be fractured, which is hopeless and only treatment is ext. Your case is probably borderline case. symptomatic without mobility. to eliminate symptoms, you can try RCT/Crown. Maybe that will last <1 year maybe >10 years, nobody can guarantee. Extracting the tooth, bone graft (will need a sinus lift for sure) and place implant may seem extreme but it’s a final fix because if RCT fails the tooth will need to be extracted and replaced w/ implant or bridge if you decide to replace the tooth. osseous + bone graft (BG) will not work because the radiolucency is at the furcation and i doubt the periodontist can place BG beneath middle of the tooth. Just because tooth has no mobility. doesn’t mean there are no problems. the tooth can have a fracture, or your filling has a leak and bacteria has gotten down to the nerve and cause problems. Without clinical exam and only relying on 4 slices of CT this is best i can help. You have to decide whether you want to try to save the tooth, more precisely, prolonging the life of this molar or just remove and replace with implant in the future. good luck
Just remove all doubt and have the tooth extracted and replaced with a 3 unit bridge. I am a periodontist and I would love treat the tooth but if you want a guarantee then you should avoid periodontal treatment and implant surgery in favor of the more predictable old school treatment. In spite of what the billboards on the interstate say implants are not a guaranteed solution
When I was doing my perio residency from 2004-2007 we were forced to read a lot of literature and perform a lot of furcation GTR procedures like this. I am not sure that I have ever heard or witnessed this scenario to be the case and in fact the science would dictate that if/when we remove the source of the problem then the bone will spontaneously fill in. If this is indeed a periodontal problem, which I doubt it is a pure perio issue, then adequately cleaning the furcation with or without a graft should resolve this “radiolucency at the furcation” and bone graft can easily be placed “beneath middle of the tooth”. I would not advocate spending the time or money to treat this unless endo was performed and by then the investment will be so high that extraction would be reasonable. I think this is a perfect situation for a 3 unit bridge.
fine nothing is impossible. lol. but is it practical? trying to perform heroic treatment to prolong the tooth. i guess that can only be decided by the patient. Literature do dictate PARL will resolve w/ endo but some PARL will never resolve after endo that’s why there’s apicoectomy.
some patients insist to hold on to their tooth and refuse extraction no matter how hopeless or terminal their dentition are. I had patients even with 1 or 2 teeth left. refuse to extract and insist on having RPD instead of complete denture.
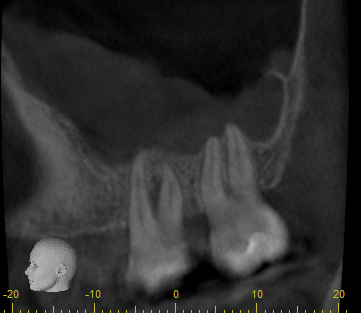
I see, thank you for your advice, I truly appreciate you taking the time. Here’s another angle of tooth 14 on the CBCT. As a non-dentist and layperson, I don’t see any PARL or periapical lesion; wouldn’t there by a black spot at the end of the root? In other words, what makes you suspect an endo problem? The endodontist at office 2 concluded no endo problem because it responded normally to a cold test
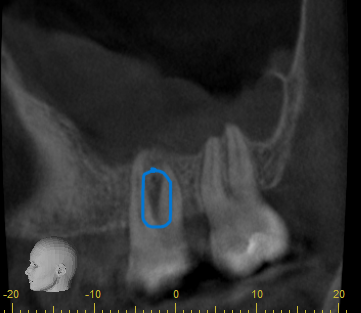
From your chief complaint. i only know your tooth is symptomatic for a few months. I don’t know what’s the problem since i didn’t perform the exam. ultimately you need to make a choice to save or remove the tooth. either root canal treatment and/or periodontal treatment could resolve your symptoms. If after you perform either or both treatments but the tooth still giving you problems, then you will have to remove. Honestly i don’t know what’s the problem with #14 but that black shadow between the roots does look different than #15. you decide to save or remove. that’s all. good luck
Absolutely I see that shadow between the root, which seems to show a furcation defect. I think you’re right; first we’ll try to address the furcation with perio, failing that we extract. Thanks again.
It is not practical, IMHO, which is why I would advocate for extraction and 3 unit bridge. While it is bread and butter “resident perio” to be performed in an academic setting it is certainly not practical or cost effective…
you should listen to Dr Scotty. he’s a very experienced and highly trained periodontist. If he recommends extraction. it would behoove you to do otherwise. The amount of money, time, energy and pain to prolong this #14 tooth outweighs removing it and replacing w/ a bridge or implant/crown. But as the patient you have the autonomy to decide. Even if you know the end result. good luck.
From my experience when dentist not sure where the infection came from, usually the tooth has unvisible micro crack, your best bet is to extract it and put an implant
Here is the opinion from a periodontist with 32 years experience. All dentistry fails eventually, some things fail faster than others. If you can afford comprehensive treatment then extract the tooth and place a membrane and bone graft, after 3 months of healing perform a lateral wall sinus augmentation. After 4 months more place a good quality implant like a SLA Straumann implant and restore it 4 weeks later. Long road but it will probably last a very long time if executed correctly.