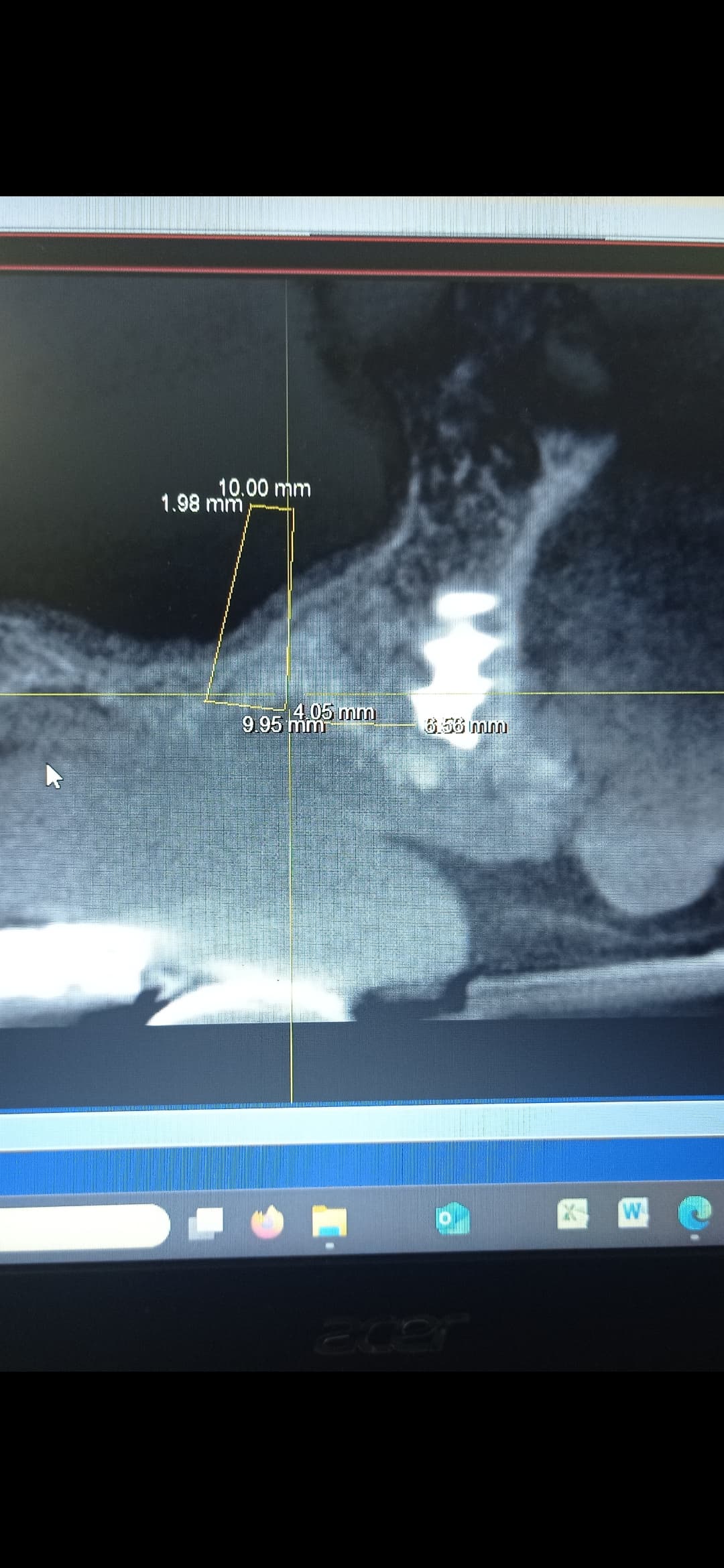
I need your opinion on this case. female patient, 60 years old, bone 4, wearing a scheletrical upper prosthesis, has 2 broken implants in the premolar canine area on both sides. The broken implants are not infected. I performed an all on 4 with tapered implant but I positioned the right tilted implant 2 mm more distally, invading the sinus. The implant insertion torque was 50 ncm. I used a removable full denture in acrylic for temporary provision. what do you suggest me to do? should I wait and monitor the situation? or I have to extract the implant?I reconstructed the position of the implant on the pre-surgery CT scan and in my opinion the distal part of the fixture is only 2 mm in the bone. In this case, is a Toronto or a bar overdenture prosthetically indicated? If I had to extract the tilted implant and the patient refused to have the surgery done again, would a bar overdenture on the 3 surviving implants work? Thanks for your attentions
yes, from your radiographs. it’s difficult to be 100% certain. but your “A” implant don’t seem to be fully in bone (best viewed w/ CT). which can cause failure when used as an abutment for a full arch implant supported prosthesis. resulting a do over. out of your own pocket since i would say is dr error.
but a few questions
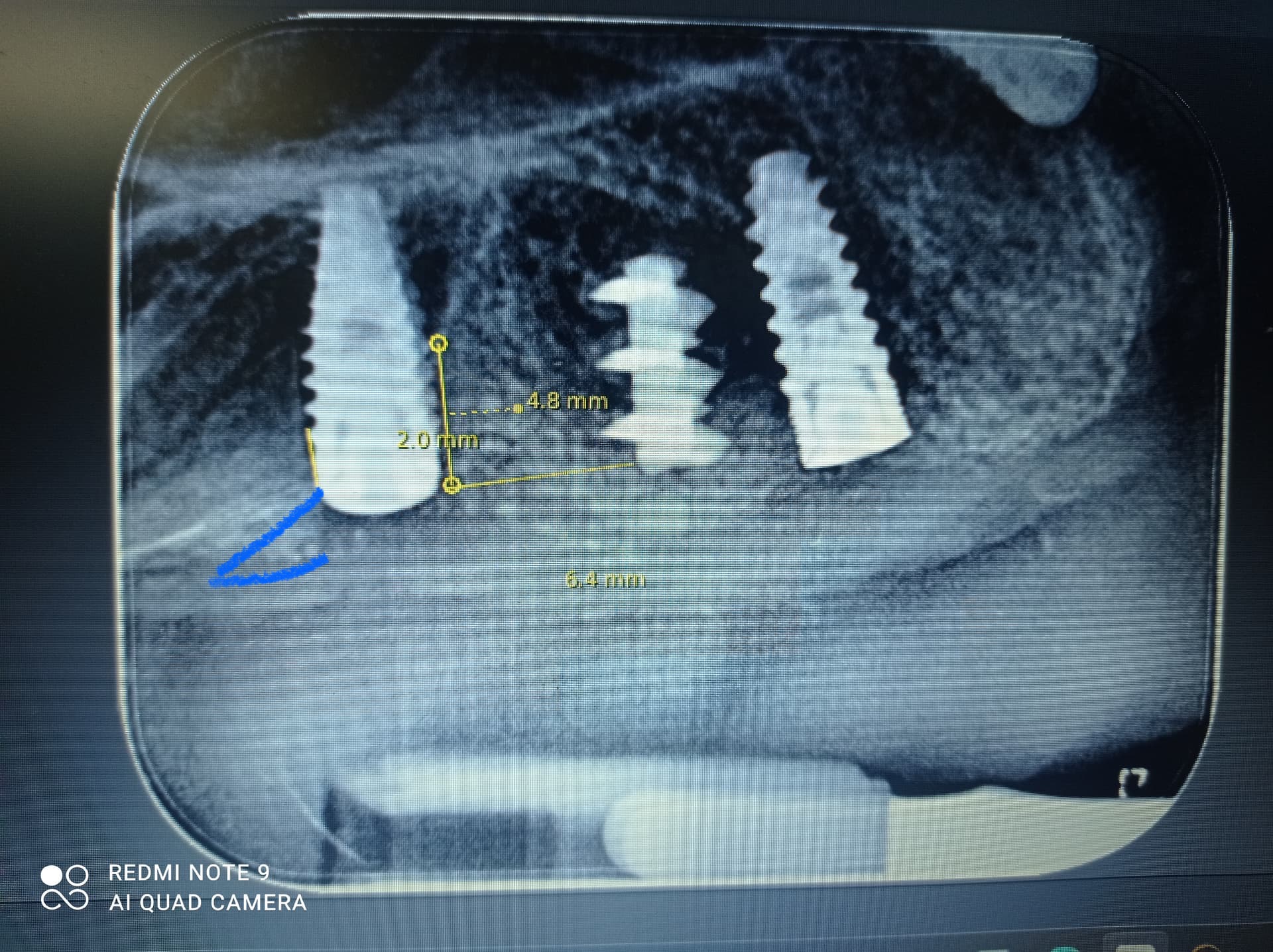
From your PAs. there seems to be 6 implants total. Why do you say 3 surviving implants? what are the 2 super apical anterior implants. Also if you doubt your “A” implant position in the sinus why don’t you take a post op CT? Using a preOP CT and drawing an implant shape doesn’t really quantify the position of the implant. And during osteotomy you should have felt the drop sensation when you went through the sinus. did you not check after osteotomy? If doing an AO4 freehand is too challenging. i would recommend surgical stent to be safe.
If you turn a FUD into a provisional. why do the implants have cover screws. Shouldn’t temporary abutments or MUA be on the implants? a removeable denture is not considered temporary provisional. A temporary provisional is you convert a removable FUD into a fixed FUD. You’re just having the patient use a removable denture while the implants are integrating, that is not a temporary provisional. If your implants all torque >35Ncm, by guideline you should be able to place a fixed provisional on the implants, ie place MUA/temporary abutments on implants, drill holes and remove the palate of your existing FUD to fit on the temporary abutments. which doesn’t seem like you did.
Also shouldn’t the decision to restore w/ overdenture or fixed denture depend on patient request and prosthesis space which is determined at presurgical planning. So if the broken implants need to be removed due to alveolar reduction. they should have been removed during implant placement.
And correct me if I’m wrong, but by textbook, upper overdenture should be retained by a minimum of 4 implants. with 3 implants only. there’s a higher chance of implant failure. but hopefully your treatment will last longer than your patient.
Best of luck.
I think many clinicians are too impatient and in a haste to place implants before designing the prosthesis (could be due to improper training or deficient experience) . I understand you feel/think once you place implants, $$$ is in and you locked the patient to your office. but lots of times after implant placement you are left worry about the prosthesis and micky mouse the treatment and pray for it to “work”. which isn’t the best method for an AOX.
the 2 anterior implants are old broken implants that the patient refused to remove. fortunately there is sufficient prosthetic space for both an AO4 and possibly an overdenture. I used a removable prosthesis during osteointegration due to the patient’s economic choice. Unfortunately, after having placed many implants, I have lost the habit of doing a ceck x-ray of the osteotomy with the pilot drill. I know the literature recommends using 4 implants for upper overdentures and not exceeding 2 mm of protrusion into the sinus but I wanted to know if clinically any of you have managed overdentures on 3 implants or implants over 2 mm into the sinus. clinically, practically, not from scientific literature. so if this were your case what would you do? Thanks for your reply
As with just about everything in implant dentistry 4 implants vs. 3 for an upper overdenture is simply a suggestion. While I have always “tried” to follow this suggestion I have, on more than one occasion, managed and even planned upper snap on dentures with 3 and even 2 implants. I have found success, and failure, regardless of the number of implants and I assume that is because I get to work with some really good restorative docs who make good dentures so these fixture are simply retaining a denture rather that supporting the prosthesis. As far as an implant protruding into the sinus 2mm I think again it is merely a “suggestion” that we shouldn’t do that and I have been guilty of successfully ignoring this one many times, sometimes intentionally. About 20 years ago I met the Becker brothers, Drs. Bill and Burton Becker, when they came to spend some time with us during my perio residency. I still remember Burt showing all of these images with implants protruding 1-2mm into the sinus and back then he was doing it for improved stability and it apparently worked well for them. While I likely failed to answer your question I hope that this is at least helpful or at least a reminder that we really don’t know what we are doing in this unregulated field of implant dentistry so the best we have is mere suggestions… IMHO we get stuck when we use textbook definitions and small sample sized case studies as gospel because if we actually knew much of anything about implant dentistry then there would likely be a lot more consistency among the materials parts and pieces associated with the craft.
i’ve placed implants 1/2 in the sinus and never had any problems before/after loading. but as for overdentures. im just too chicken to only use 2-3 implants for retention especially with my Asian pt pool. their bone just too soft and too thin. i don’t want to risk having an implant failure and having to redo the entire denture or housings. when patients pay over 10K they dont like it when prosthesis or implants fails. Even when they are using only insurance money not paying out of pocket.
there’s so many variables with implant dentistry. i think guidelines are a good ruler to atleast provide clinicians a boundary and limit. Doesn’t mean you cannot cross the boundary.
but if your “A” implant does fail (doesn’t matter why). this AO4 prosthesis would be expensive to redo or replace.
I think a better topic of discussion would be the potential cause of the 2x fractured fixtures in this patient. In my experience a fractured fixture is something that I have rarely come across, 2-3/year maybe, so to see two in the same patient would raise a red flag for me… Maybe this is not the ideal candidate for an AOX…
The fractuted implants are two “tramonte implants” that the patient received several years ago. These implants were common in Europe until 15-20 years ago but are prone to issues, especially when the prosthetic load Is not properly distribuited. Personally I have seen other fractuted tramonte screws or Scialom needles as well.
So they are low quality devices and we need not be concerned about “why” they would fracture under “normal” load? Drive on with your plan and the patient should be better off in the end!!
I have no experience whit this kind of implants. They were one-piece implants with a very aggressive design, a small diameter, and always require immediate loading. Often they were placed in flapless surgery. In the past they were made of grade 2 titanium. I think they are no longer on the market. I wouldn’t be surprised if some of the latest innovations in implantology prove to be as unsuccessful in the long term as this kind of implants. What do you think about custom subperiosteal implants? Implants companies try to sell this solutions as myraculous but i don’t know…
Internal hex implants should not be placed subcrestally, or you will get crestal bone loss. I believe that the right posterior implant will fail and when it does it will probably be displaced into the sinus. I would personally remove it.
The fractured implants could be left sleeping if they are asymptomatic and not infected.
I would place 2 or three more implants and give the patient a fixed prosthesis.
A subcrestal internal hex with a decent connection can be placed subcrestal and can be expected to experience no more crestal bone loss than an ex hex. That is unless some sloppy connection like a knock off of the old tri-lobe is used but any decent product out there today should not be a problem. If crestal bone loss is that big of a deal then tissue level implants should be used because they have the longest history of preserving crestal bone yet very few clinicians will use them because they require a little extra skill to properly place. I think it is impossible to predict with any degree of certainty that the implant on the right “will fail” and “be displaced into the sinus”.
Respectfully disagree. The literature is written, internal hex connection implants are a less stable connection than conical connection implants. There is very little bone on the distal of the right posterior implant. Because it’s a subcrestally placed internal hex connection, there will be some crestal bone loss. Then that implant is failed. Maybe it’s not displaced into the sinus. Maybe it’s stabilized in the tissues before it’s removed. I was just making the point that it may be easier to address it now before it becomes worse. Our biggest complications come when we ignore small complications. Please read Tomas Linkevicius’ papers on Zero Bone Loss Concepts.
I have read the text that you reference and I agree that a conical connection has demonstrated superiority when it comes to preserving crestal bone. I disagree that crestal bone loss is a sign of absolute failure and I say that with confidence because I see successful bone level flat top connections in folks mouths every day. Internal hex, crestal bone losing fixtures, were the standard for many years and while they might be flawed they are in no way doomed to absolute failure, regardless of what some textbook says.
There are plenty of times that internal hex implants get 1 or 2mm of bone loss, and the it stabilizes. We call that stabilized crestal bone loss. In the example show above, 1 or 2 mm of bone loss will 100% lead to failure of this specific implant.
We can get stable crestal bone with an internal hex implant if the platform is placed Supracrestally AND there is 4mm of tissue between the platform and the free gingival margin. Neither is true in the example above so there will certainly be some bone loss, and there is no room for that with so little bone on the distal. Every word above is factually supported by the literature. You don’t have to believe it if you don’t want to.
I wasn’t trying to argue, just trying to give some advice. The vast majority of implant success and failure can be known by just looking at the periapicals. If you want to learn how to diagnose this yourself please try Dr. Ahmed Mataria’s course in implant Prosthetics.
Avoid maxillary subperiosteal implants!! The bone is too soft for them. Note that these 2 fractured implants speak to implant overload. What caused it? Likely parafunction or an inadequate # of implants. Keep in mind that everything you do surgically, is something that whoever restores the case counts on. If the foundation is questionable, then you are setting the patient up for problems. All-on 3-MAY work in the mandible long term, yet the only way I would want it in the maxilla, is in the premaxilla, splinted together with a full palatal coverage overdenture. Retention only.