Hi,
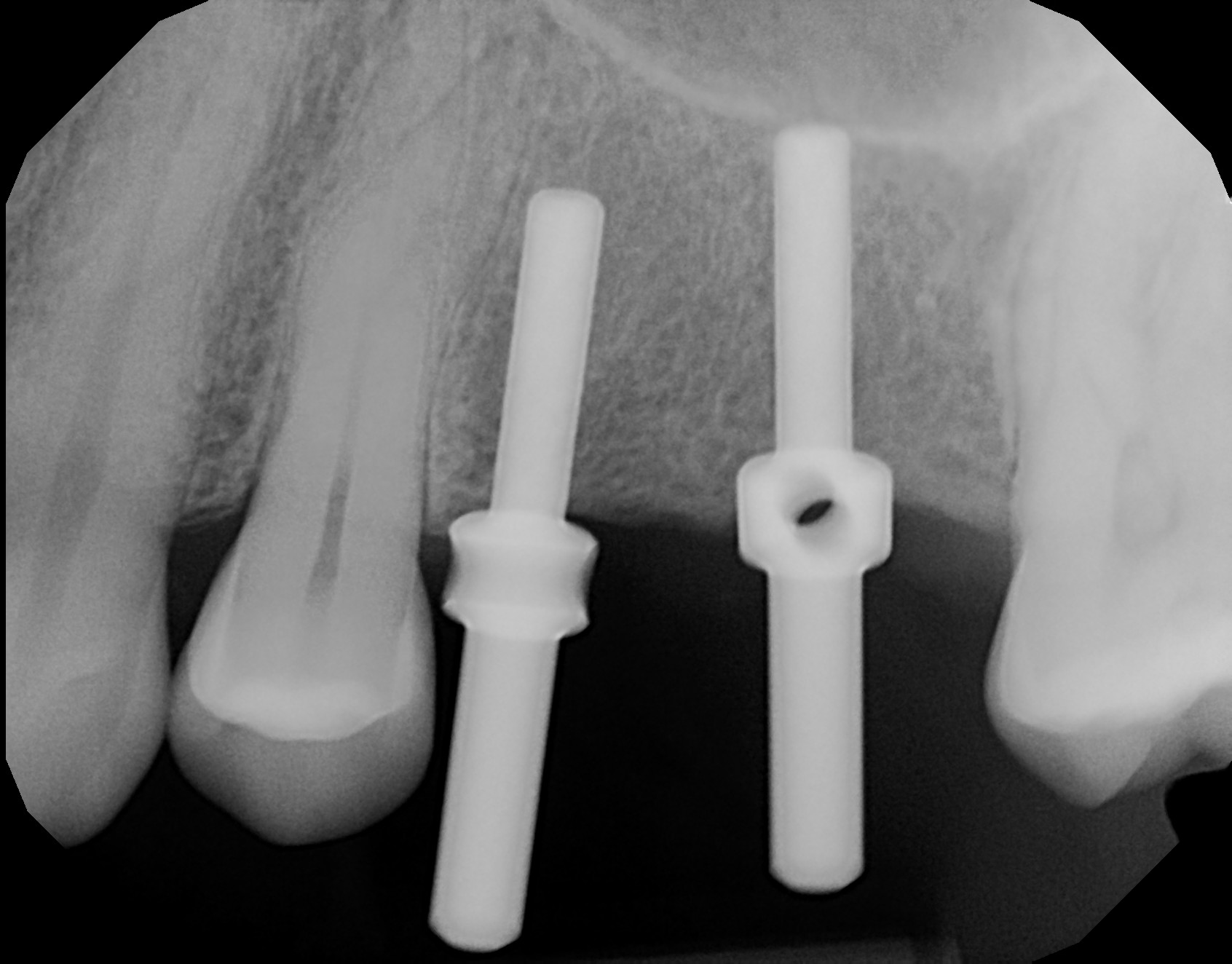
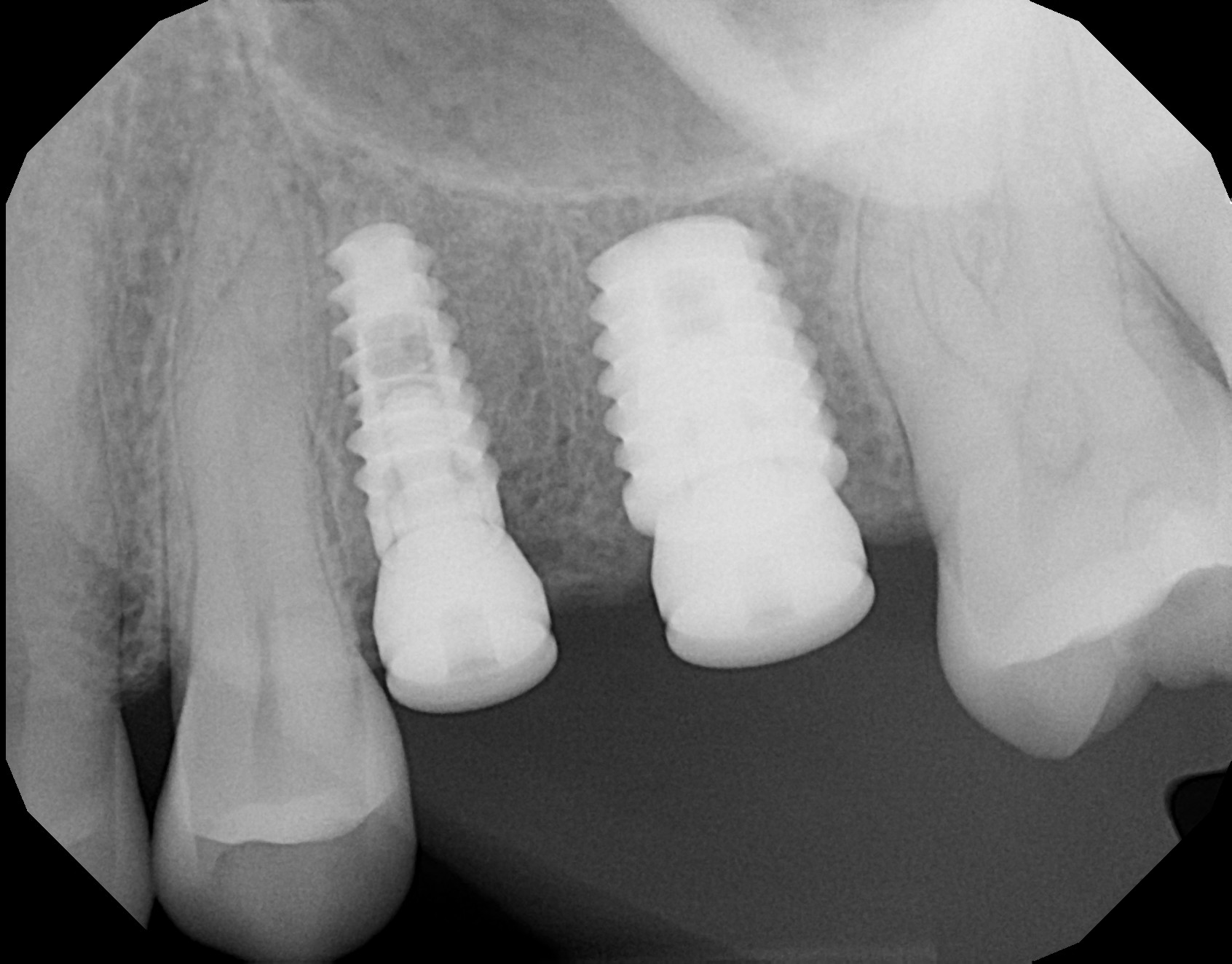
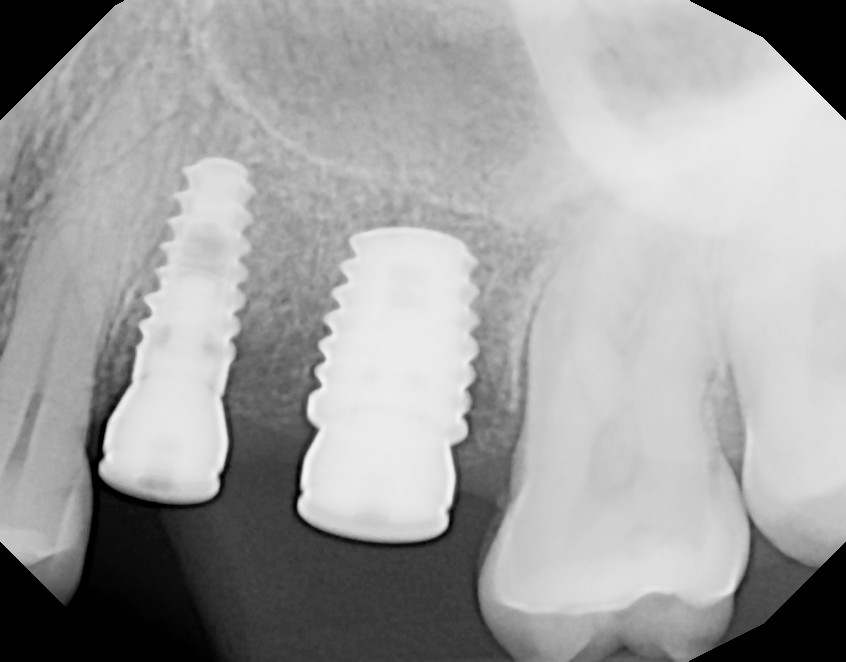
A patient had two missing teeth for several years on the upper maxillary, and I placed both implants on #13 and #14. The implant on #14 failed immediately post-surgery.
The bone height on #14 was 8mm and the bone width was between 6 to 4mm
I placed simultaneously the bone graft and the implant (5.8 x 7.5mm).
The patient started with complications immediately post-surgery: wound dehiscence, infection, and bone loss. I cleaned the infected area, added more bone graft, and put the patient under antibiotics. Three days after cleaning the infected area, the bone loss continued to progress on #14. The implant threads were visible.
I am wondering if I drilled too close to the maxillary sinus, or if it was wiser to do first a bone graft procedure. Any suggestions on the root cause?




Erich George comments:
Possibly overheating of bone and/or too wide an implant. Maybe a 4.6mm wide implant would of worked better in this site. Just a guess.
Dennis FlanaganDDSMSc comments:
The teeth may have been failed endo with an E faecalis infection that can vegetate intraosseously and quickly colonize a new foreign body (implant)
Dr KG comments:
1. Immediate placement is always high risk as those colonies are highly active, no matter how good you clean
2. The open healing protocol involves always a risk of infection/poor healing as well.
3. It is not mentioned how much the torque was to place that implant. If 30-40 ncm wasn't achieved you looking at implant loss in lower density bone during healing process
As you see risk factors accumulated here.
Tim Carter comments:
Just bad luck…
Sometimes in spite of our best efforts s!@? Just happens
Greg Kammeyer, DDS, MS comments:
Certainly a 5.8mm wide implant doesn't fit in a 4-6mm wide ridge. The bone should be 2mm thick on each side buccal lingually for predictability. I suspect the VERY thin bone became avascular because of how thin it was
Michael Giesy DMD comments:
The width of the implant caused buccal bone dehiscence most likely. You want at least 2mm on the buccal or augment with some bone grafting.
Tim Carter comments:
I see some interesting comments and they are likely all true though I still believe you should attribute this failure to just bad luck. One thing to consider is that there is really no reason to use an implant wider than 5mm. I actually never use anything wider than a 4.7 Zimmer TSVM. Unless more recent studies suggest otherwise the wider implant actually have a higher failure rate suggesting that they cause overheating of the bone. If I were to make a suggestion it would be to simply exchange your wide implants for a slightly narrower option and work on achieving better wound closure (not that it caused the failure but for style you can get better approximation) and with practice you can trade those PTFE sutures for something resorbable.
Jaime Ramos comments:
I purposely place my implants 1mm into the sinus floor for increased primary stability , so this was not the cause . You are placing 2 implants to support 2 crowns , so 2 NP implants would suffice . Implants need space M-D & Bucco palatally in this case . Sink your implants 4 mm from the Zenith and this will help with primary closure .
Z Khokhar comments:
Thank you for sharing your case. Failures are not inevitable. They can happen even to many experienced surgeons for different reasons.
I admire you for asking these questions. That is how we learn from each other.
It seems from your questions that you do not have much experience placing implants.
Have you taken any good surgical as well as implant restorative courses. Also it will help if you can find a great mentor.
It is a suggestion. Please don’t take it in a wrong way.
I have been doing implants for many years and yes I have failures too. It good to learn from one’s mistakes. If any tells you they never had a failure, they have not done many implants. Unless their patient passes away. Then it is 100% success rate. Unfortunately, that has happened to me.
Learning never ends.
Aquiles Mas comments:
Seems like bad luck man. It’s happened to me. One case I know I overheated the bone. The other case was an immediate. I’ve done these Cases all kinds of ways. And sometimes it’s just bad luck.
alan J comments:
Anytime you add another variable ie bone grafting to placing an implant, you increase the odds and risks of something unforeseen happening.
There are inherent risks just with straight forward placement .We can only speculate as to what happened , as no one knows for sure why your case went south.
Anyone who does implants will have failures and those that tell you that they don't have failures are either lying or don't do them. One of my golden rules is that I try to have at least 2mm of native buccal bone around the implant
Keep doing what you're doing and learn from each case so that your next case will be better
CONAN TENG DDS comments:
You mentioned bone graft. These were edentulous sites. So where did you place the bone graft? did you do a veneer graft on the buccal of #13, 14? 4-6mm buccal/palatal width of alveolar ridge is kind of on the thin side but acceptable. With a 8mm sinus floor and 4-6mm width alveolar ridge. vertical sinus lift would have been a good option to place a 3.7-4.2mm diameter and 11.5-12mm long implant. I agree with Dr Kammeyer. Possible your 5.8mm was too wide for your alveolar ridge. also #13 implant looks awefully close to #12 root. but then again, sometimes implant just fails. there is a 5% or less chance of implant failure.
Mahi Bagur comments:
Plenty of reasons for failures, main one is ' Bone is not holding or gripping the implant '. I read the comments with interest, all of them are contributory on their own accord. Minimal prep, self anchored, completely submerged implant would have given better results. Best wishes for next time. Out of curiosity- does any body do -Basal Implants.. ? take care.
Robert Teague comments:
Maybe not so in this case but two other reasons for early failure often overlooked are the use of blunt or damaged drills. Avoid overuse, undue pressure or poor handling at the cleaning stage. The other is vitamin D deficiency. With something like 1 in 3 deficient, its an easy chair side test to rule out at consent.