Dear colleagues, I have placed an immediate Straumann bone level implant in position of upper left canine, restored it 4months later. The implant is quite deep. Almost a year later the patient still feels discomfort. I suspect bacterial accumulation at crown implant interface giving slight pressure and discomfort. I have tried bulking buccal porcelain and even switched to a provisional adjusting anatomy but symptoms persist. I am now thinking of explantation, allowing healing and reimplant 4months later at more crestal level. What is todays protocol on explanting a fully integrated implant. Kindly advise. Many thanks in advance.
Dr AG comments:
Please post xrays of the case and clinical picture. Implant can be reverse torque, if not possible, piezo around or trephine but will create bone lost. It is very case dependentJean Paul Demajo comments:
.545911461642173250Ecg3Kt1NKOhtWPvQFiDW.jpeg)
Jean Paul Demajo comments:
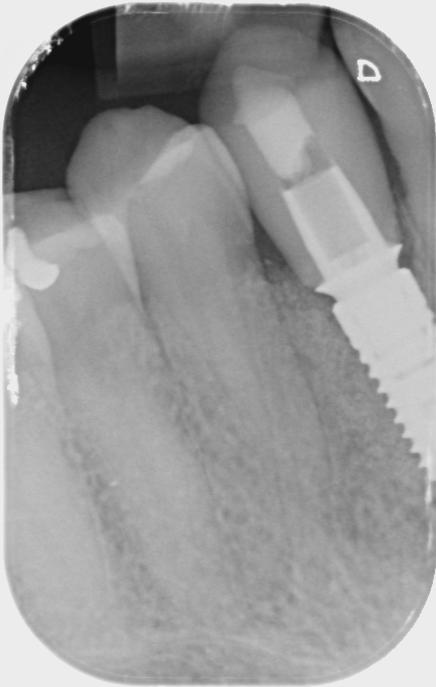
The lateral incisor seems close but there is an element of beam angulation and superimposition. The lateral is also Not tender to percussion.Jean Paul Demajo comments:
Paul Newitt comments:
There seems to be very little room for soft tissue at the crest level of the implant. What appears to be a Ti base abutment appears subosseous. Is that the case or film angulation. Have you attempted removal of the prosthetic and back to healing abutment to see if symptoms abate? You may want to re evaluate emergence profile here. Photos would help as radiograph images can be misleading.Rob korman comments:
I agree with Paul regarding lack of interproximal space which would lead to insufficient interdental papilla creating an esthetic disaster if the peri-implant tissue is revealed in smile line. I would recommend to remove the stock abutment and fabricate a screw retained PMMA crown to see if you’re able to develop sufficient peri-implant tissue that is acceptable to the patient before proceeding to a definitive restoration or thinking about removal of implant. Have your ceramist crate a flat to negative emergence both facially and interproximally in this particular situation.Jeffrey Backer, DDS comments:
Hi. If you explant using piezo or trephines you will undoubtedly cause much damage to the lateral. Make sure your informed consent is reviewed by a lawyer. What is the nature and extent of the patient's complaint. Pain scale 1-10, constant or intermittent? More noticeable on awakening (ie brux/occlusion)or later in day, chewing make it worse? swelling? Percussion ( not only implant but multiple teeth crossing the midline), pulp test (adjacent tth crossing midline consider going from #6 thru 13 skipping #11). Triple check occlusion looking for lateral interference on left lateral excursion. What size implant was used, did you use a CBCT, was it guided surgery or free hand, Did you take a follow up CBCT considering its symptomatic. Maybe you perforated the buccal plate, palpate? Consider a referral for a second opinion before you go down a potentially troublesome path. Does the pt brux? Sometimes there is referred pain, I would like to see more than an isolated periapical. The problem is most likely the too close proximity to the lateral without a minimal 1.5 mm space. And either the nerve or the bone is compromised. If you do elect to remove consider having an oral surgeon explant, graft and ultimately place another implant (your expense), and you can restore. Curious, as it was an immediate implant was it immediately provisionalized, how? Were the symptoms from day of immediate placement of implant or only after the 1st 4 months? I would never restore something that was symptomatic. Lastly could be the dreaded.... Bill-itis, was the case paid for at the time of surgery or before? Hope this helps.Jim Curlin, DDS comments:
Before you do anything more drastic, try changing the Abutment to a longer Collar, where your margin is just slightly below the gingiva. Then, make a new Crown. I'll bet that will solve your problem, and stop the pain.Guest comments:
Please check the implant abutment interface. Try restoring with a long gingival collar. Agree with Dr.CurlinDr. Jozef Šesták comments:
Do not explant. Implant is good oseointegrated. Remove crown, abutment, make new, individual one ,in cad cam system if doesnt exist fabricated, with longer insert part to move connection (colar)in the gingival level coronaly. Because it is esteticaly exposed field, use zirconia for abutment ad crown too.CONAN TENG DDS comments:
Explant can be easy or difficult. Easy as in using a wrench and just turning it counterclockwise, or difficult when you trephine or just using a surgical handpiece and FGSL701 going around the implant and removing enough bone until you can unscrew the implant. Which I have done it all. I noticed you used a stock abutment. Try have your lab fabricate a screw retained "custom" abutment crown. Deep implants with using stock abutment with 1mm collars can induce "discomfort". When using stock abutments. Drs usually does not specify collar heights of the abutment. But if you did provide your own abutments perhaps you should have given the lab a higher collar height stock abutment. like 3 or 4mm collar. Your provisional is still using a stock abutment with a short collar. Try a custom abutment. This should help your patient with his symptoms. Also the implant looks super close to upper left lateral, but so far no bone loss is seen on your radiograph. When you mention discomfot what kind of discomfort is it? Can you be more specific? clinical pics would help. how about probing? BOP? purulence? inflammation? hygiene? Explant usually is the absolute last option, unless there is class 3 mobility to the implant or severe bone loss. Then the implant will explant itself given time. Good luck.Jean Paul Demajo comments:
Good afternoon all. I have removed the crown and placed a healing cap. Within a couple of hours the patient experienced immediate relief. I will leave it with this healing cap for a month or so and then take an impression for a new crown raining then platform to 1mm below gingival level. Thanks again for your help and guidance.