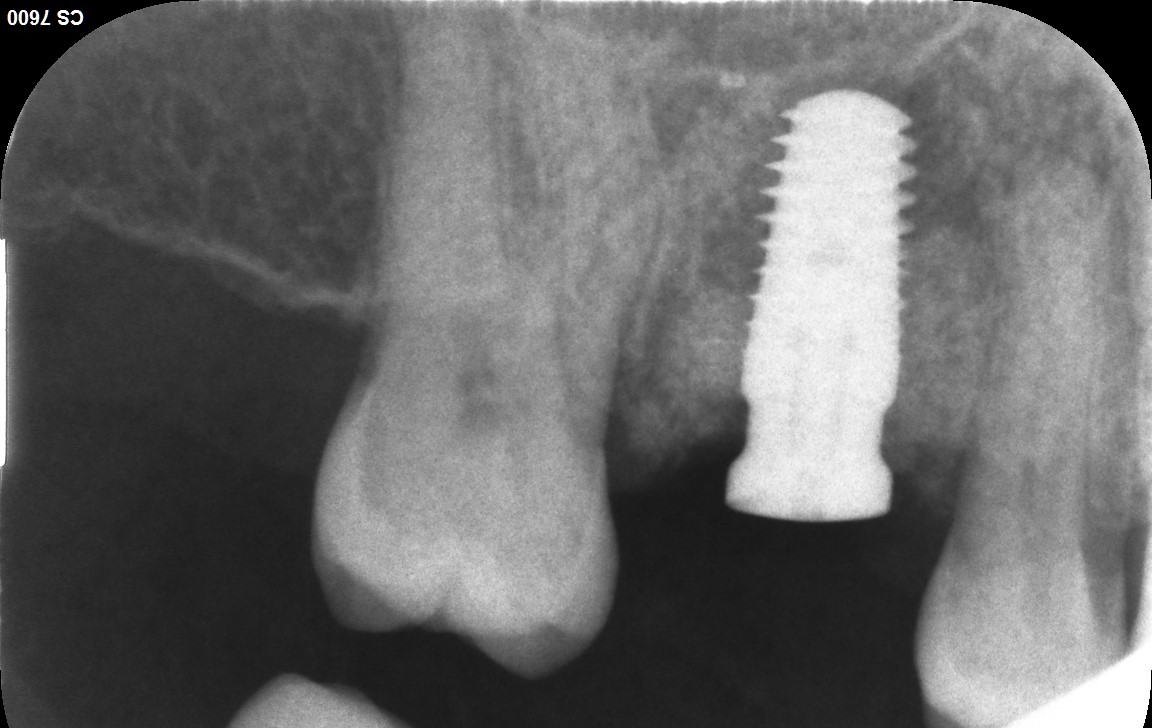
It seems as though most folks are still opting to utilize a staged approach when replacing molars, especially maxillary molars. My preference is and has always been to minimize, within reason, time and cost for my patients. About 15 years ago I started placing immediate implants for maxillary molars and can honestly say that it is equally as successful and predictable as the more tedious and expensive staged approach. Attached is a case where #3 was sectioned and extracted with the immediate installation of a 5.4x10mm ZimVie TSX with an Encode healing abutment at the time of placement. The peri-implant void was filled with NovaBone putty and 2 simple interrupted 4-0 Chromic Gut sutures were placed to reapproximate the tissue. I prefer a putty as it stays well contained even without the use of a membrane and the soft tissue will rapidly migrate over the exposed portion of the putty. This is a relatively simple and predictable procedure that has been incredibly beneficial for me and my patients alike…

Good placement, job well done, Scotty.
scotty, why didn’t you use a parallel tissue level implant (ie, straumann TL)? thank you.
I have come full circle as a result of the error of my ways. For years I completely abandoned the device in favor of the more one size fits all tapered bone level but I have come back around. I still use ZimVie most of the time but have learned from my past mistakes to lean in favor of the tissue level for posteriors… I wish I would have used tissue level for this case but I was still learning…
Truth is I got in bed with Zimmer and let it go to my head and I utilized only their stuff for years. I like their stuff and I think it is among the highest quality in the industry but along the way I kept seeing my old tissue level cases come back looking great. I contacted ZimVie and was put in touch with the R&D folks who informed me that the current market does not support the investment in a TL fixture so I gravitated back to Blue Sky Bio One Stage. The better question is “why did I ever stop using the BSB One Stage” and the answer to that question is “My Ego got me”.
How can an easy implant in natural healed site/bone be more expensive than immediate implant+biomaterial? Immediate implantation is not a easy one. Many use implant guides, not to slip from the correct prosthetic position in sometimes narrow septum, most use biomaterials of different origin to fill the voids of alveol, some also ad CTG. And the idea of immediate implantaion is not only to place a fixture, but equally important is to manufacture an individual socket seal element, abutment or a provisional crown, to keep the soft tissue architecture. So faster ok, but not easier and for sure not cheaper. My 2cents.
All great points though the majority of my patients work and understand the value of their time so reducing the number of appointments is a huge savings. I have always found it much easier to properly form an emergence profile when working from a fresh site rather than a flat native ridge so in my experience immediate placement makes more sense, when practical. I have never embraced the use of a surgical guide for single tooth cases and especially not a single tooth immediate and I have always considered the use of supplemental biological materials to be part of the fixed fee for an immediate implant with no tacking on of additional fees. I can certainly understand that if a punch list approach to dental/medical billing is used then it could get expensive but aren’t most of these materials going to find their way into a properly planned and staged out conventional/delayed approach to implant placement making it just a drawn out expense rather than a one time fee?? In the end I guess it depends on the situation and the individual provider’s comfort zone but I have found immediate placement to be beneficial and result in improved patient satisfaction. I suppose it also affords them more time to enjoy their investment but it is not always practical or possible so by no means am I advocating for it as a one size fits all approach
Thanks for your case presentation. I have been doing immediate implants for over 25 years for the same reasons you mention. For molar replacement I have had excellent success with wider diameter implants (Southern or Keystone). The reasons are: the increased diameter of these implants negates the need for simultaneous grafting; the wider implant platform improves the emergence profile of the prosthetic components, decreasing the embrasure space making the hygiene more like natural teeth; and the aggressive thread pattern ensures excellent stability at insertion. Though I still do not recommend immediate provisionalization, my experience is restoration can proceed as early as 2 months post-op. Ridge preservation grafting is one of the most over used procedures in implantology.