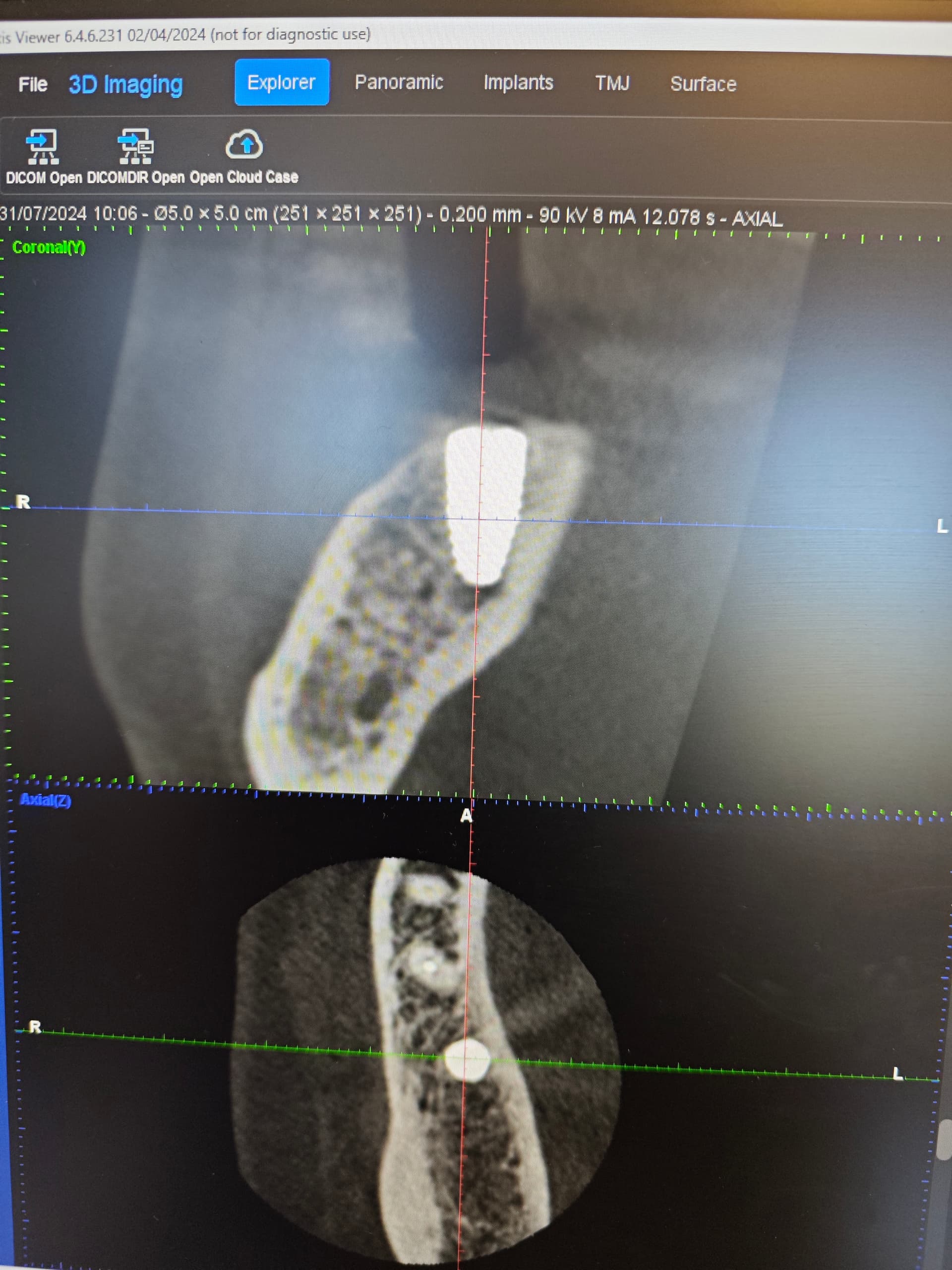
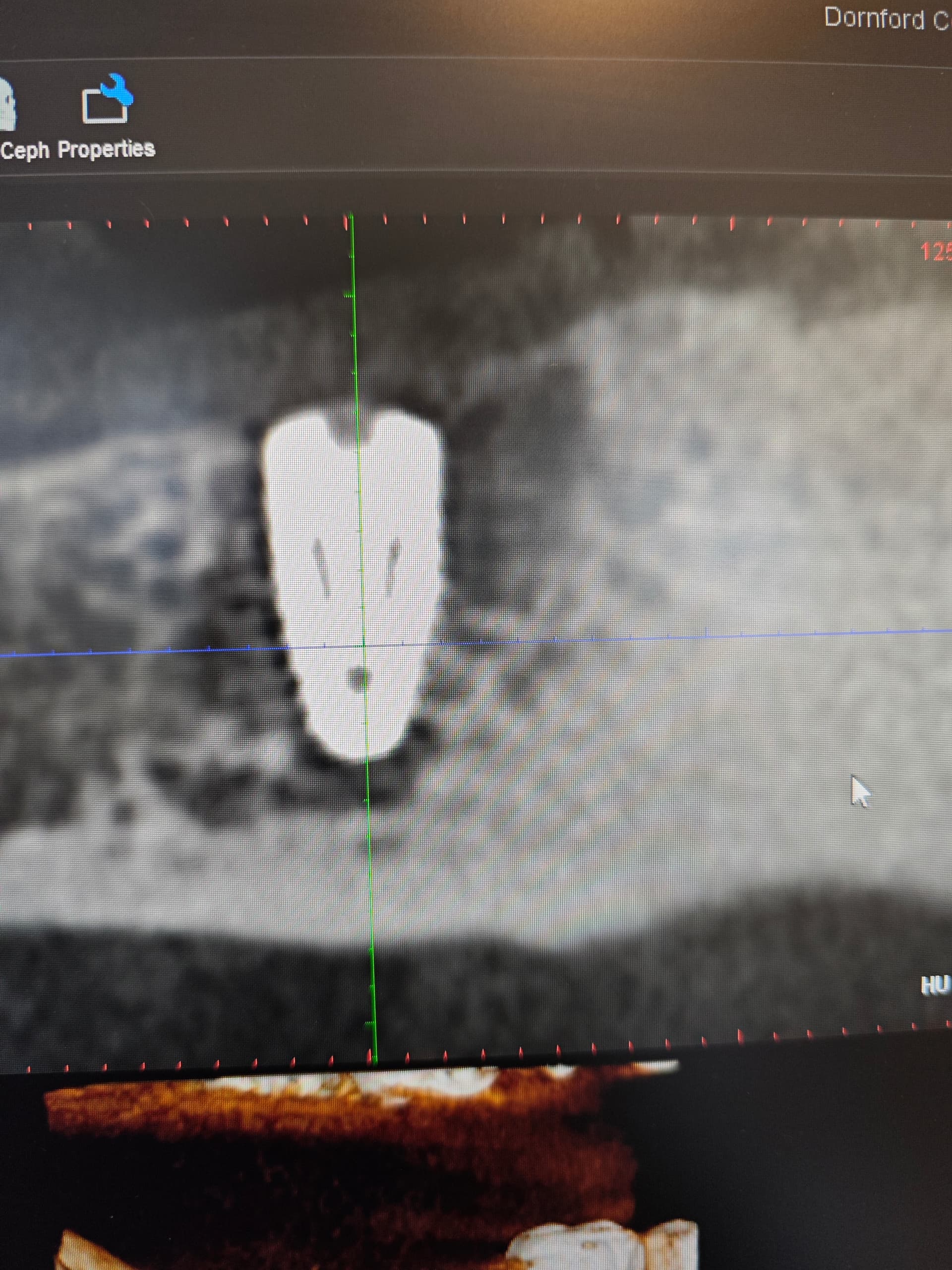
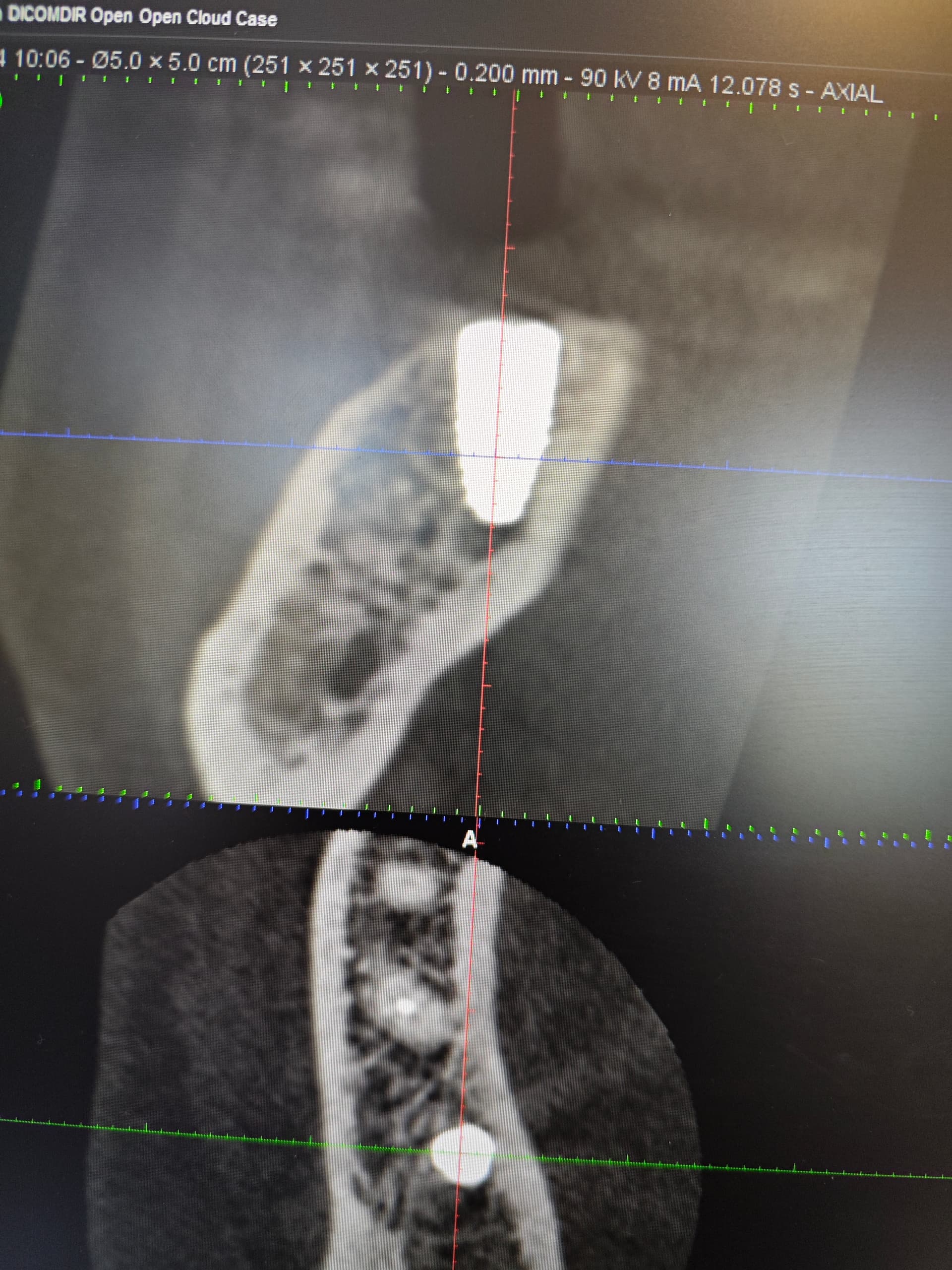
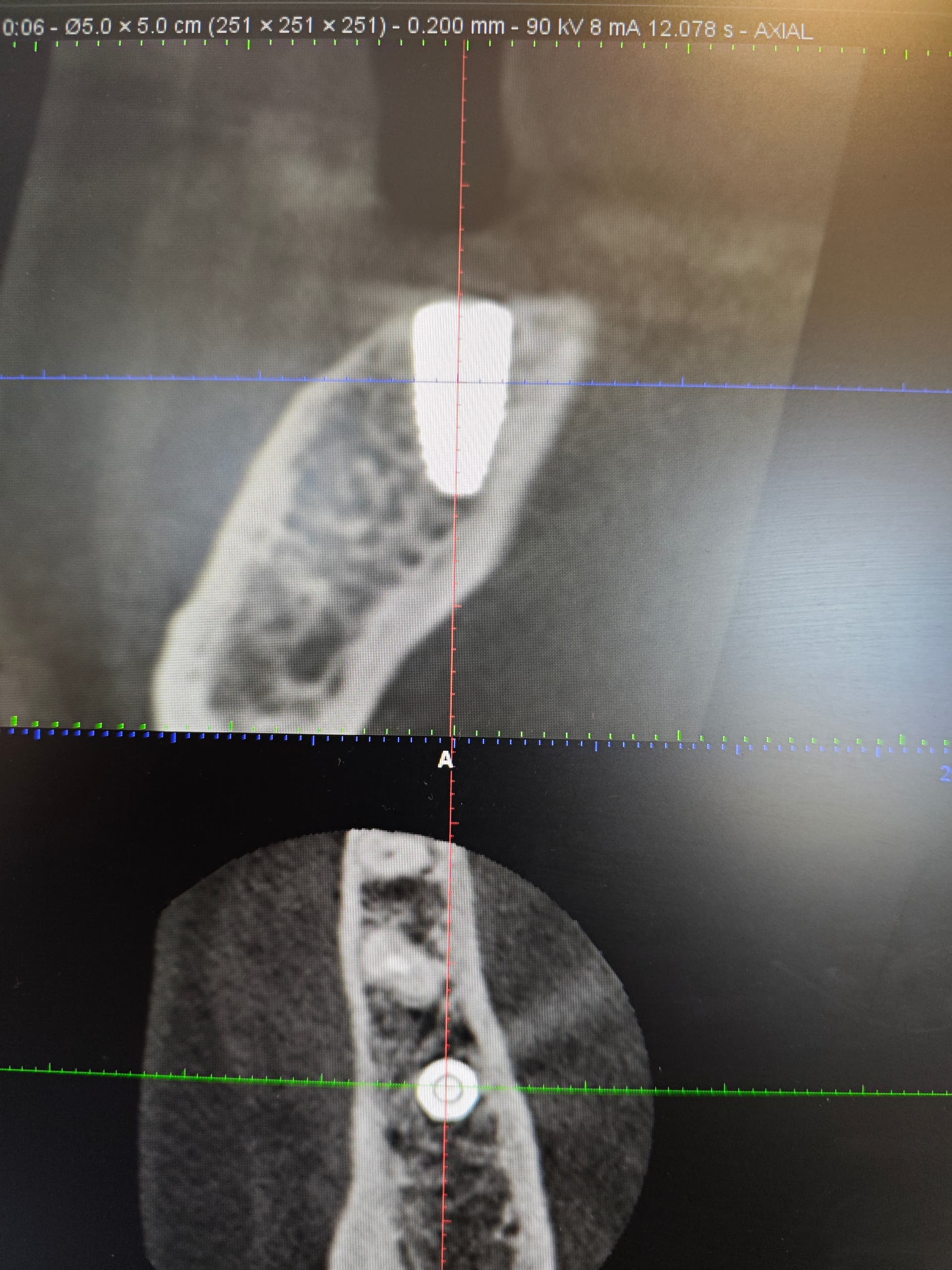
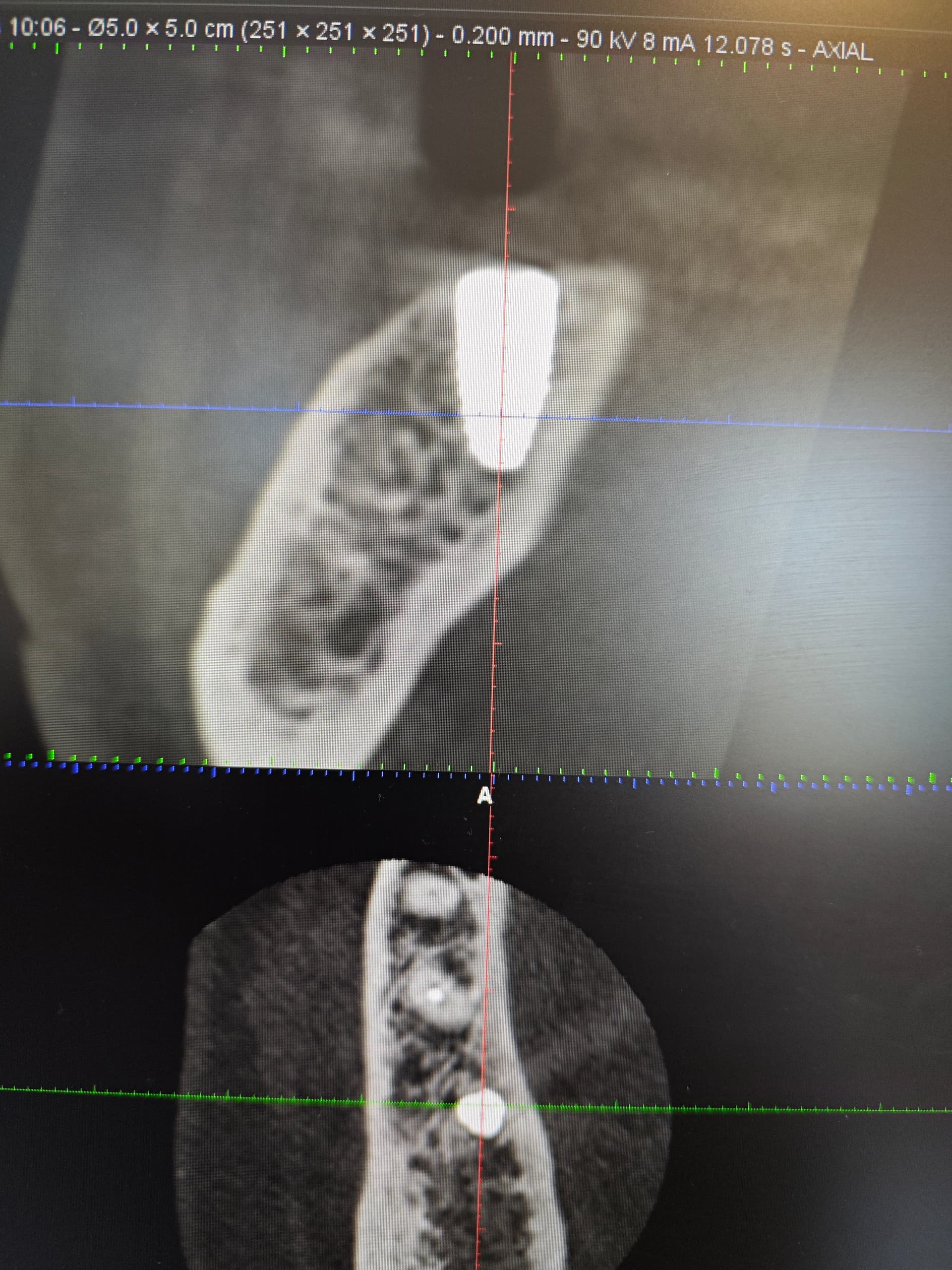
A straumann implant placed 2 months ago may be failing, personally havent seen the patient myself since placement but the referring dentist informed me patient is starting to experience ‘something’ which she wasn’t before. Clinical photos showed possible swelling on the lingual but dentist informed me that was not fluctuating and was firm. He didn’t notice anything concrete. I sent the patient for a CBCT.
Not sure what the apical void is ? Just trabecular bone. Also I guess the adjacent tooth isn’t in great shape.
Out of interest moving forward when I have have created the osteotomy site for the implant, if it isn’t placed all the way to bottom of osteotomy is that problem ? I assume a blood clot will form and achieve bony infill ?
While some might opt to criticize the placement I will say that everything looks fine except that you might just be experiencing an inevitable implant failure. While it is common for “studies” to boast tremendous success rates for dental implants reality would suggest that the complication and failure rate is much-much higher than what gets reported. Keep placing implants and you will see for yourself that sometime failures occur despite our best efforts. As for the apical void… yes it will fill in and no I would not concern myself with it.
Thanks for your reply, I tried to place the implant prosthodonically driven but found the bone morphology slightly tricky.
As mentioned I haven’t seen the patient personally since placement, it was a submerged implant. In your opinion from looking at the CBCT would you agree it’s failing or it’s difficult to ascertain until clinical investigation ?
I have seen so much variation in radiographs that I would never condemn a fixture based on a picture. It might very well be failing and if it was placed 2 months ago I would go ahead and uncover it. I rarely submerge an implant fixture and instead place a healing abutment on the day of placement. I adopted this philosophy based on my long term success using tissue level/one stage fixtures (Straumann TL, Blue Sky Bio One Stage). Unless there is a removable appliance or some esthetic concern I never submerge fixtures as the most successful implant fixture of all time (Tissue Level) was designed from its inception to be exposed and never submerged. Over the past 2 decades I can honestly say that I have experienced more complications and failures with implants that I submerged and treated in two phases vs. those exposed to the elements from the day of placement. If I were to suggest anything it would be to trust the fact that implants do not need to be submerged and there is actually more documented success with non-submerged fixtures. At any rate open it up and see how it is because if it is failing I would rather know today than a month from today…
As far as “prosthethodontically driven” placement I assume that means you planned the case and used a guide. Oddly enough back 20 years ago when I was a perio resident and we trained in the same clinic as the prosth residents we were required to place every fixture with an analog guide designed by a prosth resident. Keep in mind that we were not afforded the luxury of routine CBCT so these guides were designed on a stone model using a surveyor. What we discovered is that this method of guiding often times placed our fixtures too upright and parallel and often times dangerously close to perforating the lingual. Interesting that in 2024 with digital planning and advanced technology that “prosthetically driven” still seems to place these fixtures upright and dangerously close to lingual perforation. Remember that a mandibular molar has a lingual inclination and IMHO should be translated to the fixture being prosthetically planned.
Thanks for all the feedback. I recently had a couple of failures which I previously didn’t and now this could be the third one in a short time span. I’ve been trying to figure out what’s changed. Things that crossed my mind
Poor sterilisation autoclave from the nursing team
Fully guided stents reducing the amount of irrigation
Not placing to the osteotomy bottom
Tapered implants
Possibly lax disinfection of the implant sites and transferring granulation tissue
To be honest I’m a bit lost to why I’ve had these failures and have been wracking my brain.
Since the previous two failed I’ve been submerging as I thought occlusal factors may be contributing on the healing abutments.
I hope this one hasn’t failed but will keep you posted.
Dull osteotomy drills either from overuse or poor handling during the sterilization process is the most likely culprit though I strongly believe that surgical guides are a factor as they inhibit irrigation and they are one more non-sterile surface touching the drill. While tapered and parallel implants both perform extremely well I do believe that some fixtures have too much taper (Straumann Tapered Bone Level, Nobel Replace, Bio Horizons…) and can lead to some unnecessary pressure necrosis. Since you are a Straumann guy I would suggest the original Straumann Tissue Level which is a parallel walled fixture and probably the most successful fixture of all time that very few folks still use. I think it fell out of favor simply because folks want something simple that can be used for all cases and tissue level fixtures require some skill to properly place and are not well suited for full arch or anterior cases.
To answer one of your questions
“when I have have created the osteotomy site for the implant, if it isn’t placed all the way to bottom of osteotomy is that problem ? “
The answer is NO PROBLEM
Having placed all type of implants since 35 yrs - I have not seen any issue with that-
You are doing good- learn from your mistakes- thats the key
question. since you placed the implant and buried it. Will you 2nd stage the implant and replace the healing cap w/ a healing abutment/collar? or the referring GP? by then you can check right?
and what is the “something” the patient is experiencing?
I exposed the implant and it was firm and placed a healing abutment. I guess that apical void was nothing of concern. Her complaint was related to almost like a lingual sequester of bone but didn’t appear to be associated with the implant. I am not sure if this bone morphology was present prior to placement and the patient can’t remember either. Thank you for the advice and reassurance.