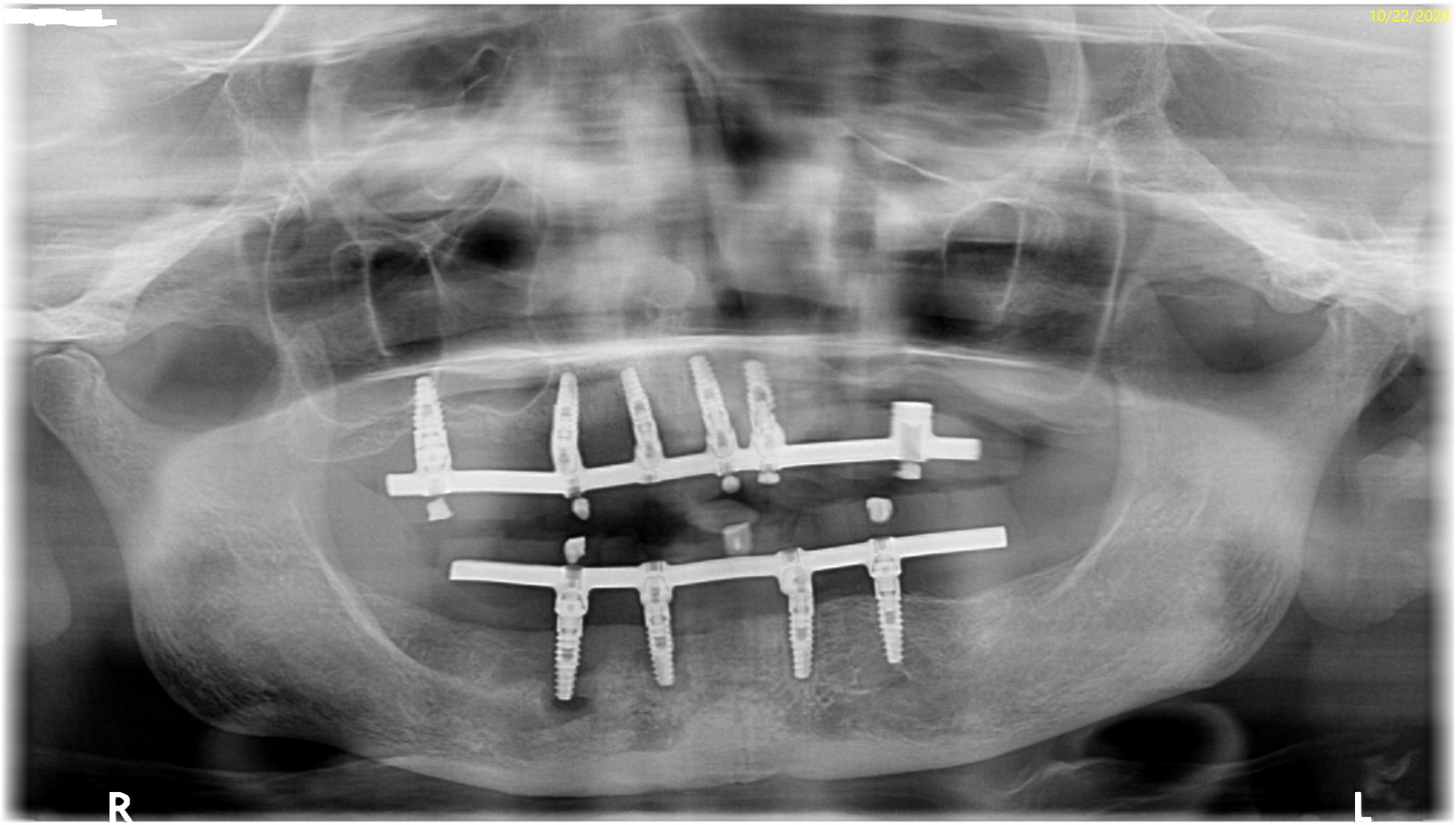
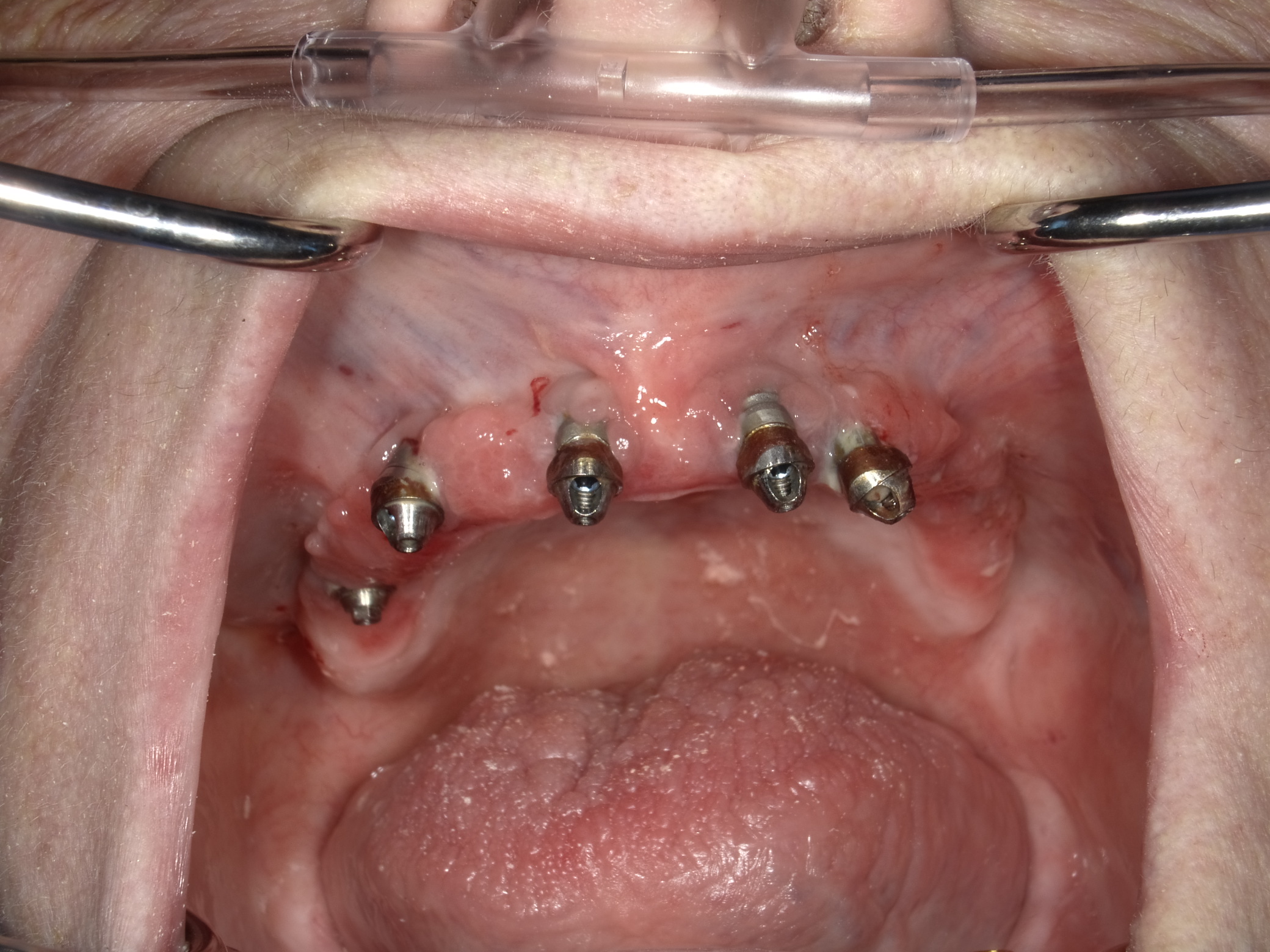
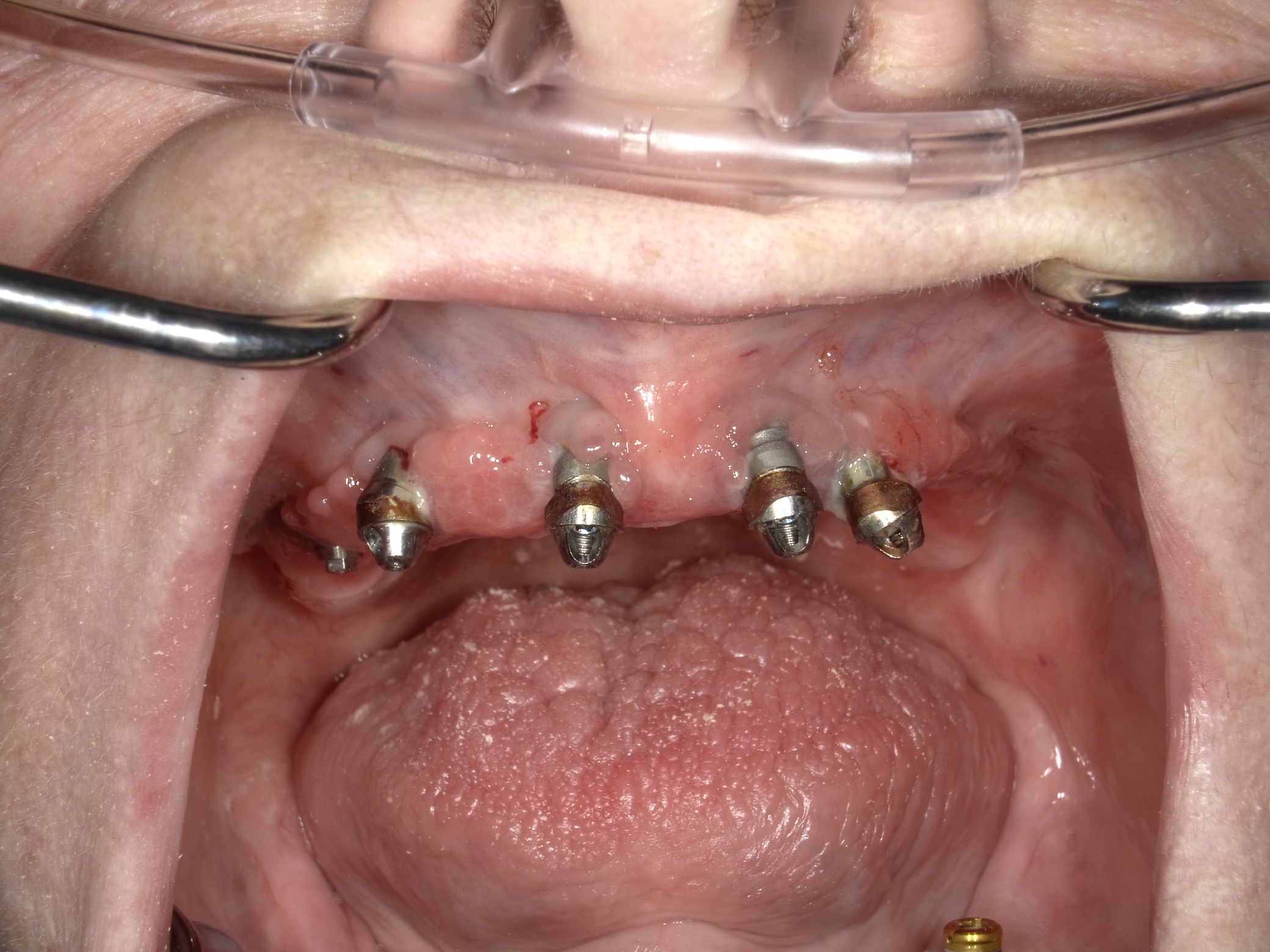
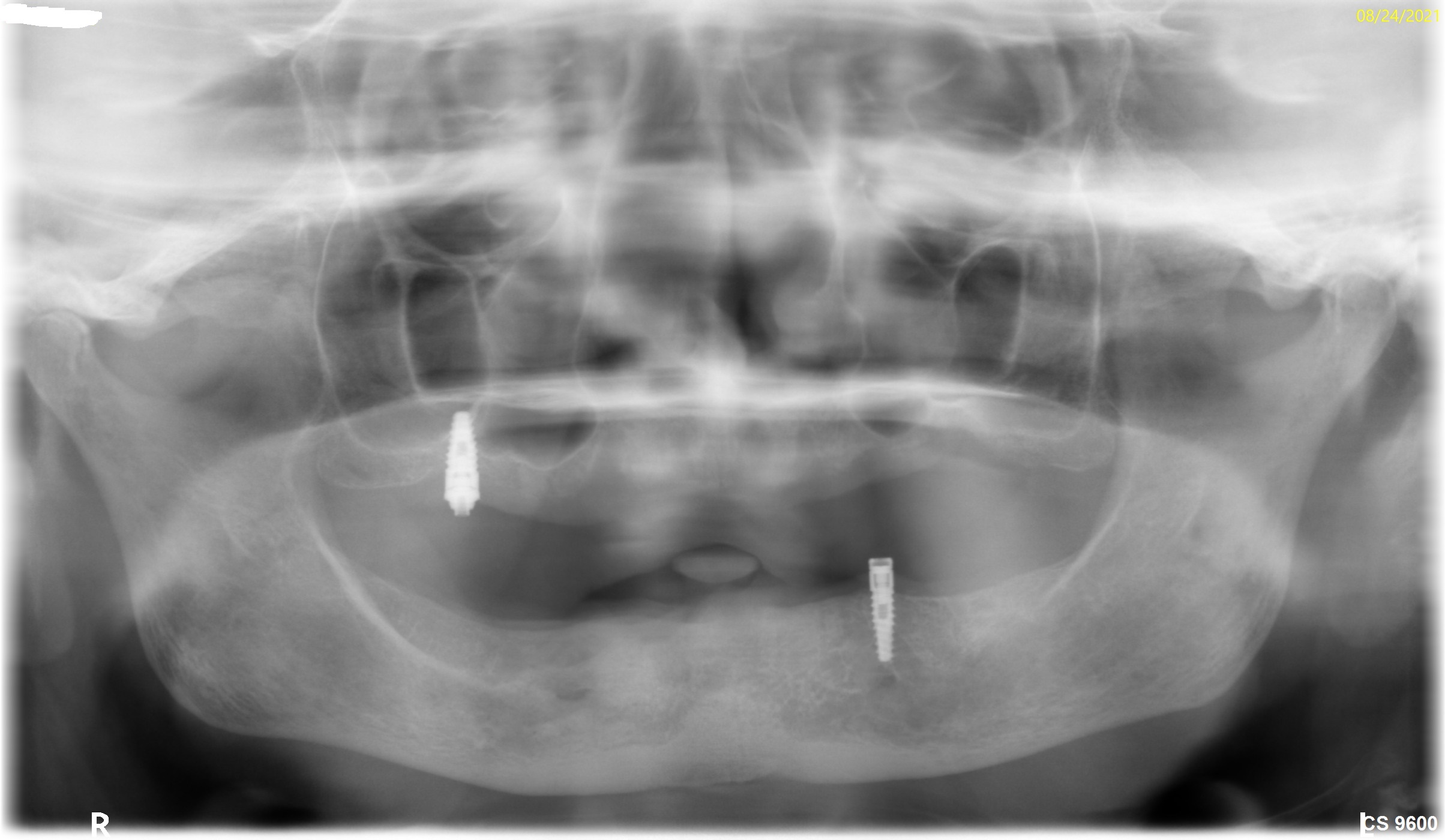
I received this case about 3-4 months ago as she was having… well she was having a lot of problems. Without going into the details because the pictures tell the story she was treated by a single provider who opted to wear the hat of both surgeon and restorative doc. As a periodontist, I have been to multiple hands-on restorative training courses, probably more than most restorative docs that actually treat these cases, but I limit my involvement to that of the surgical member of the team. I just think that problems like this can be prevented if we all stay in our own lanes and practice a Team approach. As one who has been involved in many of these cases I am convinced that this treatment concept is best done with a 3 member team of Surgeon, Lab, Restorative doc, and for best results at least 2 members of the team need to know what they are doing!! In this case, clearly, both arches failed and I am showing only the upper along with the fractured implant removed from the #10 area.


Curious comments:
I’m unclear… was this a restorative failure, or a surgical failure? And, are these two procedures (Ao4 surgery and Ao4 restoration) so complicated that no one doctor can possibly have adequate knowledge of both? I’m assuming the surgery was done incorrectly, since you (a periodontist) are managing the complication. What would you have done differently?Timothy Carter comments:
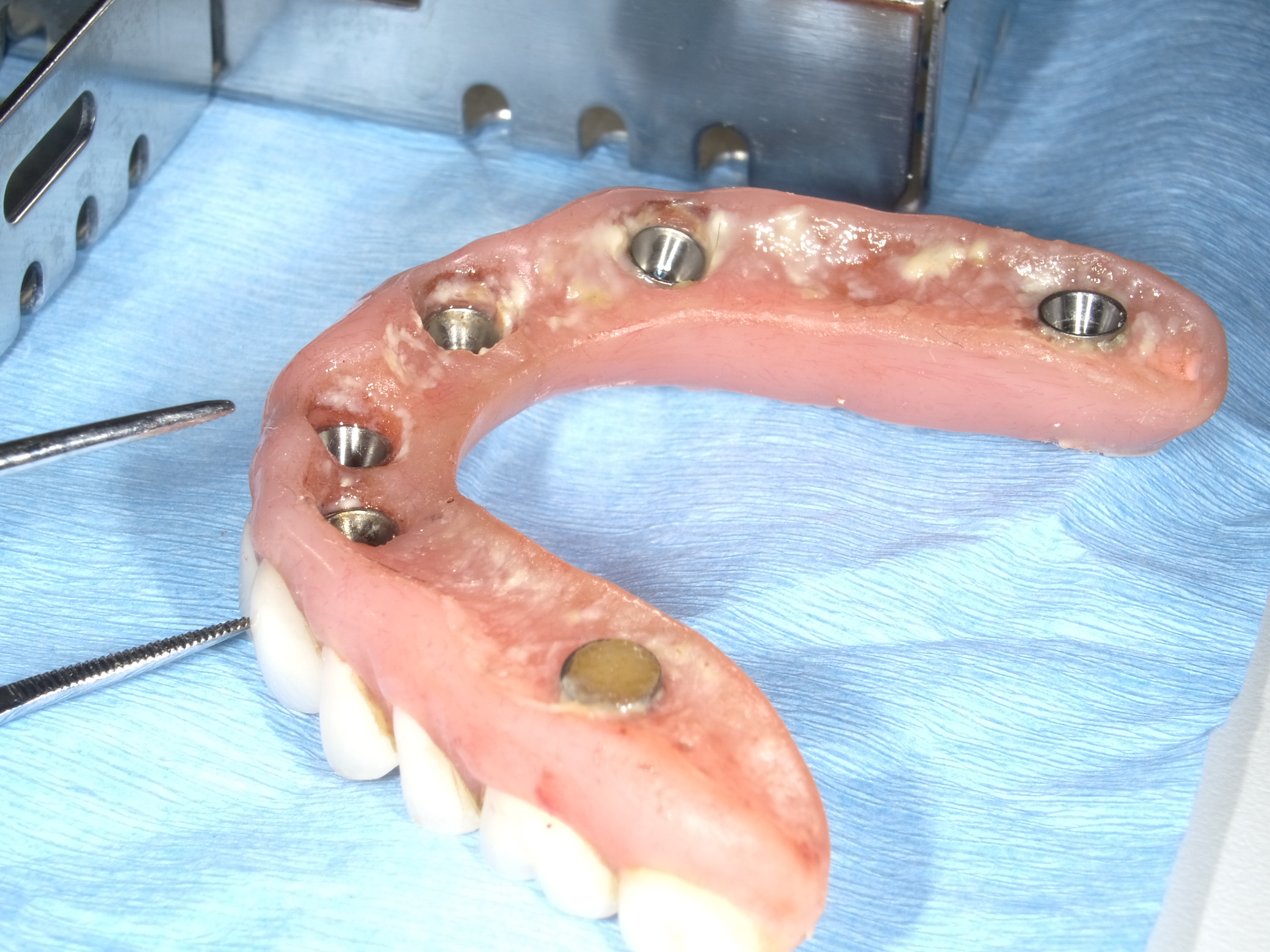
For starters look at the intaglio of the prosthesis and you tell me…Timothy Carter comments:
I would consider this a failure to planNeil Bryson comments:
I’m finding it difficult to agree with our periodontist here. I did my first implants in 1984, been in practice since ‘75. I started doing implants BECAUSE OF a periodontist. He sent four anteriors back to that were so poorly angled and improperly spaced that we had to go back to ground zero for a restart of the case. I have also had oral surgeons place single implants in areas of scalloped ridges, or in areas too close to the buccal and lingual plates without a thought as to the future ability of proper oral hygiene. Perhaps it was my fault in not being more assertive as to the results I expected. But, let’s remember here who we are talking to…THE SPECIALIST ! It is difficult for the young practitioners to be assertive with those who are on alert constantly protecting their turf with their “superior “ knowledge. Your idea of a team approach is exactly what we need but SO difficult to cultivate. I will also take exception to your argument of the intaglio surface. We have all had appliances just like or similar to this that have been in service for 25 to 30 years with NO problems simply because of good hygiene and regular recalls. We generalists who have the ultimate responsibility as the quarterback of the “team” should guide the surgeon depending on the restoration required. I maintain that a generalist who is not trained to do surgery should probably not refer an implant case to a surgeon If you don’t know the limits of surgery then you shouldn’t be thinking about restoring a case. So many of our specialties in this area have been doing their own restorative on the implants which I feel is a violation of Board rules. Some are acceptable cases but a few are not. Instead of pointing fingers you should be delicately and patiently engaging your referring dentists and offering your services and guidance. But the guidance should be at a time and place to discuss the case WITH the generalist and not just send it to me and we will talk. Until the specialists respect from whom the patient initiated and understands our responsibility, I will still prefer a generalist who can do and understands surgery to do the entire case.Matt Helm DDS comments:
Excellently stated! I always appreciate your comments, but never more than this particular one! You are absolutely right in all respects, especially that we GP's are really the quarterbacks of the team, because none of the other players have the whole combination of training and skill-sets that we do and, cannot see the whole picture like we can. Personally, I cannot see what exactly would qualify a periodontist more than a GP to place implants. Most periodontists don't have adequate restorative training, and cannot visualize the whole case in ensemble. If the business card says "Practice Limited to Periodontics", that's the lane periodontists should stay in. Like you, I too have seen enough failures from them. Excellent comment Neil. You hit the nail right on its head in all respects! Absolutely excellent!z comments:
Very judgmental of you. Patient had several implant failures in the presence of obvious bad home care, probable comorbidities and periimplantitis that is unpredictable. There are plenty of cases like this that are successful, and many that fail regardless of who the 'team' is.Timothy Carter comments:
Not judgmental at all as I have been adequately trained in all aspects but understand the concept of TeamTimothy Carter comments:
Do you think that the ridge lap on the prosthesis might be a factor in what you call poor home care. This case was poorly planned and a 3 member team would have eliminated that factorHerman Comlekci comments:
3 member team vs 2 member team vs 1 member team? It makes no difference if all the members fail at some step in the treatment sequence. Clearly the Lab is somewhat responsible here as well. Lets not forget the patient must share some responsibility in these failiures as well. I've witnessed patients SMOKING right after Implant Placement Surgeries. It is important though, the treating clinician educate themselves prior to tackling cases such as these. Just a thought!Matt Helm DDS comments:
Nonsense! I've seen 3 member teams do cases like this worse, and I've seen excellent GP's do a better job alone! You can't generalize, nor should you! If you're fixated on the 3 member team because you don't have the prosthetic training or talent, that doesn't mean that everyone is the same. The fact is that there are many well trained and very talented GP's out there that are worth an entire 3-team. You're being too judgmental, and perhaps simplistic of this case, whose reasons for failure go way beyond just intaglio. It looks like there was also very poor patient home-care. A case like this never fails for one reason alone, but due to a multitude of reasons. Your presentation narrative was much too short and too lacking a complete history and many important details to be able to even begin ascertaining what went wrong, where and when. One thing is certain, there is no one-size fits-all, and everyone, even the best have an occasional failure or mishap, sometimes due to factors that are out of their control. Here's a good analogy for you. Did you ever hear the saying that in Indy or Formula racing the very best drivers put it into the wall with absolute regularity? It's the same here, sort-of.Spence comments:
You state that as if the 3-member team is infallible...and always outperforms teams of 2. (Pretty much nobody does the dentistry AND the lab work from beginning to end, so there are no 1-person 'teams'.) It can't be all about the face bow and articulator. I wish you'd state exactly what you see as the problem and what should have been done instead. Why would that have lasted so much longer?Pros doc comments:
As a prosthodontist I too get to retreat train wrecks caused by the under educated overly confident super dentists. Unfortunately, super dentists don't generally listen to specialists. They are usually good advertisers and smooth talkers so we specialists have a difficult time combating this trend. Until our implant companies and special interest groups that teach weekend courses ( often in foreign countries) for big profits take responsibility for creating these problems we specialists are pretty much relegated to doing damage control. And in my state, our dental society is useless in disciplining these offenders.Dennis FlanaganDDSMSc comments:
I think it’s time that our profession stops these judgemental criticisms without a helpful analysis as to why a case fails. We all have failures. None of us has a perfect record. While I agree some of us go beyond abilities but it would be far better to find the causes of the failure for our own edification.Timothy Carter comments:
If you can’t tell how poorly planned this case was just by looking at the intaglio then there lies the judgement. A 3 member team would have eliminated this critical error of restorative spaceSmyledoc comments:
You KNOW that was the cause of failure? Wow your knowledge really is advanced. Tell us how you can know that.Spence comments:
Without a doubt, this was a 2-member team. Even the skilled generalist has the lab make the prosthesis. Isn't your actual point about planning? In hindsight, what should have been done that was not done? (And don't simply say "planning" :smirk: ) What do you see when looking at the intaglio that tells the story for you?holden comments:
A significant component of my practice is managing ailing and failing full arch cases. Obviously the one case you show had both surg and restorative issues, but your suggestion that cases done in one office--regardless of the flavour of dentist providing the tx--have more or less problems than cases done in multiple offices, is simply not true.There may be practitioners out there that think their particular specialty or practice model is superior, but experience does not bear that out. We see cases from everyone and everywhere.
What is true is that when a case with multiple providers involved goes south, it can be difficult to get someone to take responsibility, and it becomes a nightmare to manage as the periodontist or surgeon will refuse to take off and re-insert the prosthesis to access and revise the area or remove an implant or whatever. It sounds like you would be comfortable taking off the prostheses to deal with this, but that is often not the case with a periodontist, and the patient winds up driving back and forth across town. Who suffers for this added complexity? Always the patient.
Timothy Carter comments:
Clearly everyone except for Pros doc has completely missed the point of this post. This case was poorly planned by a single clinician and a team approach would have eliminated the obvious reason for the failure. Look at the intaglio and it tells the reason for the failure. It should be smooth and convex, never rough and concave… not enough space. The individual that did this happens to be a good restorative dentist but refused to use a team and overlooked the obvious.Guest comments:
GP’s should stay in their lane!