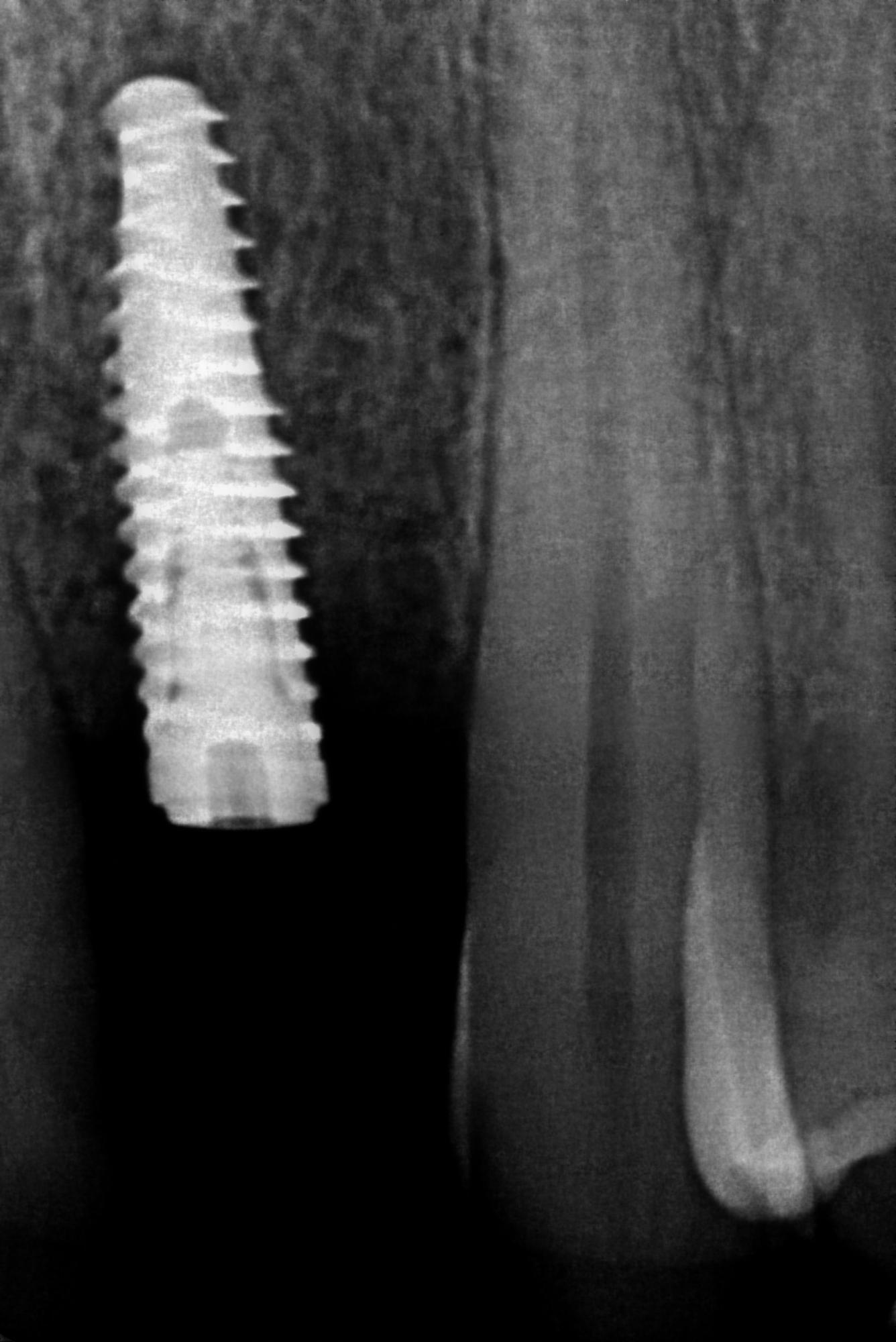
I placed this Neodent- immediate placement, 22, about 6 weeks ago. I am happy with the prosthethic position but was a bit buccally difficient with bone on the post op CBCT. Grafted with coral xenograft and placed a membrane.
Patient has an abscess now- at site 24/25. Patient was given Augmentin 5 days by his dentist, as I was out of town. I plan to open and drain it tomorrow. Im not sure if its the graft material that somehow migrated.
The flap seems to have dihiscence, and I think I lost the bone and membrane. My concerns are the bone loss, the recession, distally, on the neighbouring 11 and the abscess of course.
After I open and drain the abscess, and I guess remove infected material. I wanted to wait until abscess free and then regrafting and submerging with an Ossix plus membrane.
How long do you think I should wait to intervene? I know that 4 months is ideal, but do you think I should intervene earlier- perhaps at 2 months, due to possibly infected material in there?
There are obviously a lot of ways to skin a cat but I would suggest going in ASAP and doing everything in a single procedure. It is most likely a foreign body reaction to a piece of graft material or something and will spontaneously heal upon removal… In the event that you need to do additional graft/membrane, etc.. I think it would be best to do at the same time that you drain it because every time you re-enter the site you are making an esthetic compromise. Just a suggestion from someone who has made a lot of mistakes in the past. At the end of the day it is either a success or a failure and doing it in multiple stages is just kicking the can down the road in the event of a failure and it is best to know sooner rather than later so that you can “fix” the problem.
What type of flap design do you suggest for this patient for the regraft? It’s a lateral incisor. Patient has a medium smile line.
-full flap?
I’m concerned if two months is enough to re-enter- and whether the existing graft will be compromised and the flap will have enough blood supply. Also- how will I close the flap? If I advance the flap- what about the perforated part of the flap?
How will I close that part if I had to do a coronally advanced flap?
In my opinion this case needs soft tissue augmentation much more than it needs bone… If when you go in to drain it it is still stable I would irrigate copiously to flush out any foreign material utilizing with a remote flap extending from the midline to 12/13 area. Harvest a connective tissue graft and secure it over the fixture and extend the graft over the buccal of the site. Again if this fixture is still solid it is best to know sooner rather than later and it has a soft tissue deficiency, not a bone deficiency, that if not addressed will lead to serious esthetic compromise. just my opinion on how to skin this particular cat.
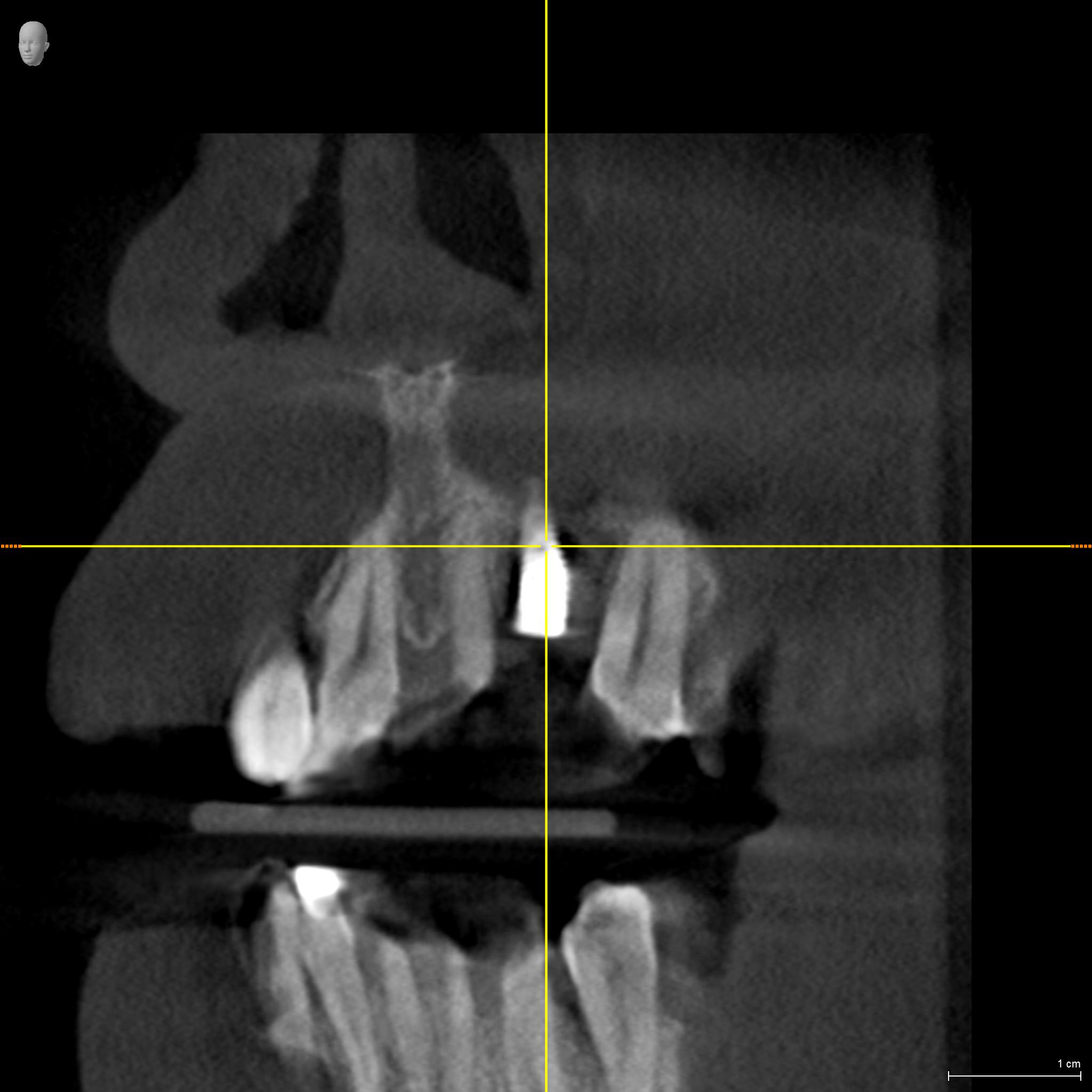
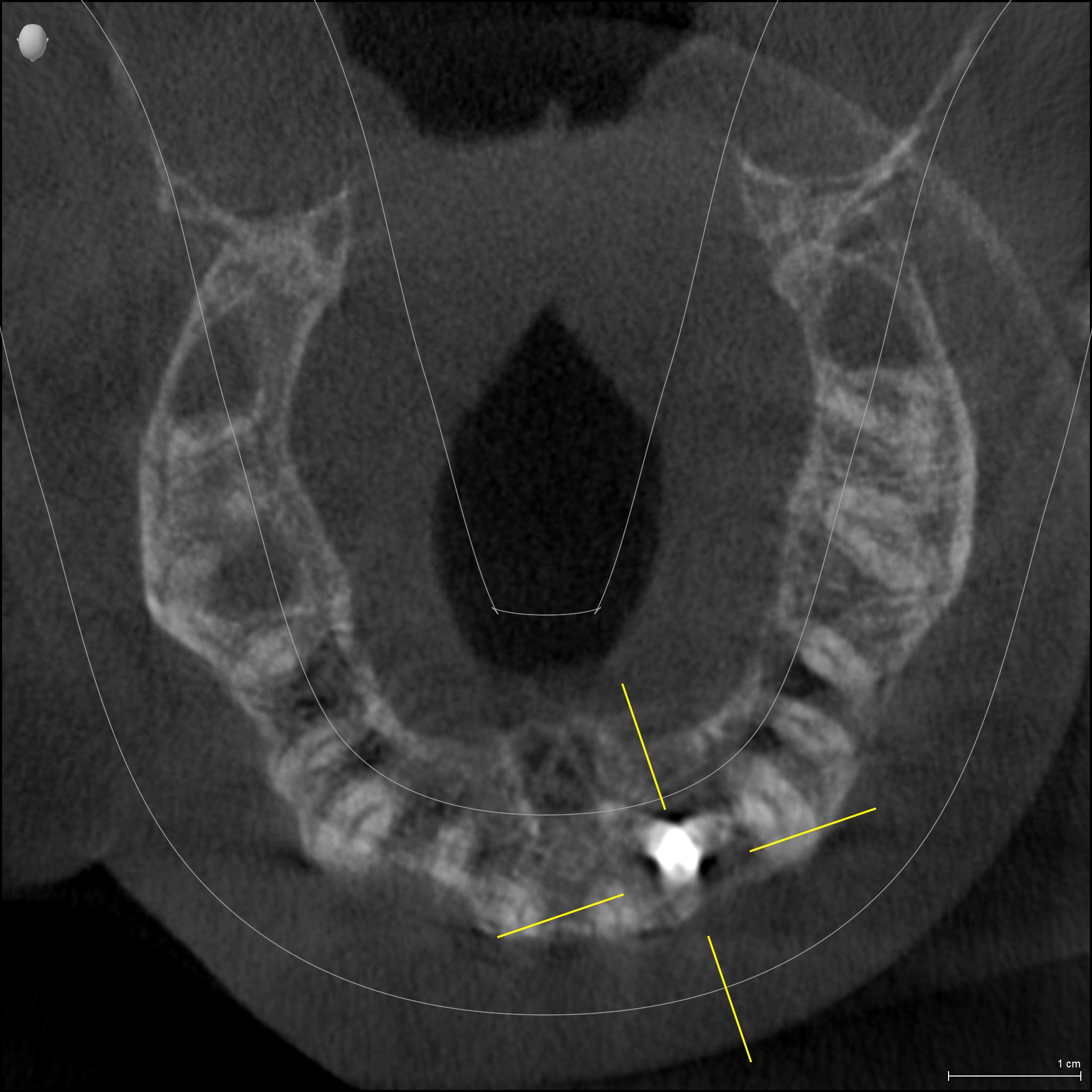
There seems to be circumferential bone loss, unfortunately. I showed it to 3 other Perio colleagues who recommended removal.
Seeing that there doesn’t seem to be bone on the buccal. I’ll try and upload CBCT images soon. Would you recommend explantation and GBR?
I’m probably going to refer the case to another Perio for a bone block and implant placement. I believe I have lost confidence in the case, and the patients confidence as well…
Lots of ways to skin a cat and taking it out is certainly an option and likely the best one available… it has yet to be determined if the fixture is even still solid. No one would argue with referring it out for removal-augmentation-and replacement. Regardless of the technique used I would suggest a soft tissue augmentation because at the end of the day it more important than the bone but for some reason we never forget about the bone … I would be a little concerned though about the mindset of anyone who would do a block graft here over the extremely predictable particulate options… Sounds like someone just returned from a course and is itching to get their fingers wet
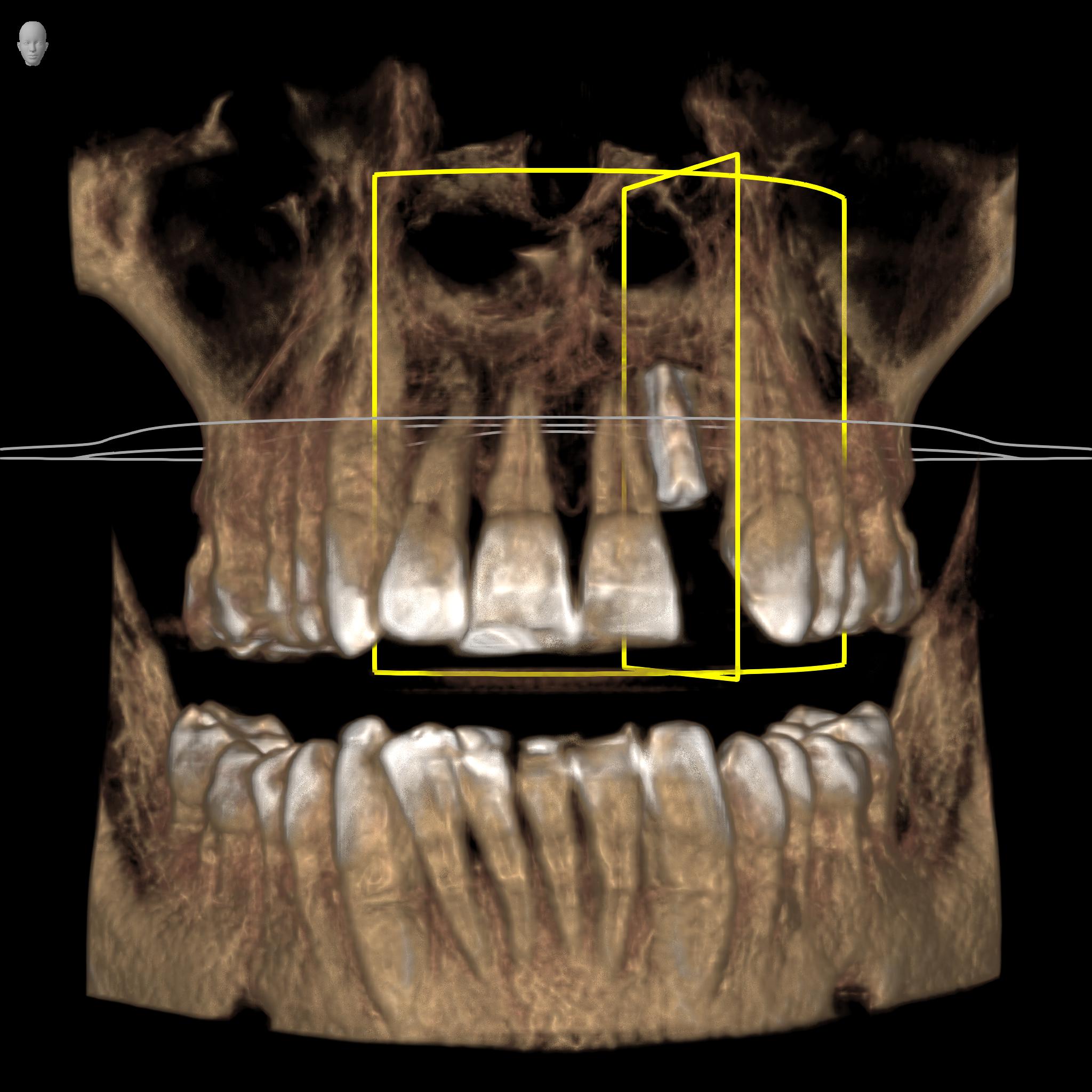
My experience would suggest that you will almost always see deficient buccal bone on the CBCT of a maxillary lateral. I would suggest getting away from using CBCT to evaluate in that parameter because it will lie to you and in the event that it doesn’t lie to you you should get used to anterior fixtures having little to no buccal bone despite successful integration. This has never been a problem when covered with thick attached connective tissue and it was never a problem until everyone started taking CBCT images and “trying” to over-diagnose. Maxillary anterior teeth rarely have a thick buccal plate and maxillary anterior implants are no exception…
As much as I would like to provide some helpful comments I am just not comfortable using information from a CBCT to make any reasonable evaluation of a maxillary lateral because the CBCT technology is still not adequate for evaluation of this area. I could make 100 different assessments based on the provided images but with so much metal interference and the inherit shortcoming of CBCT I will just concede that it looks like every other cluttered up CBCT image and I have no idea…