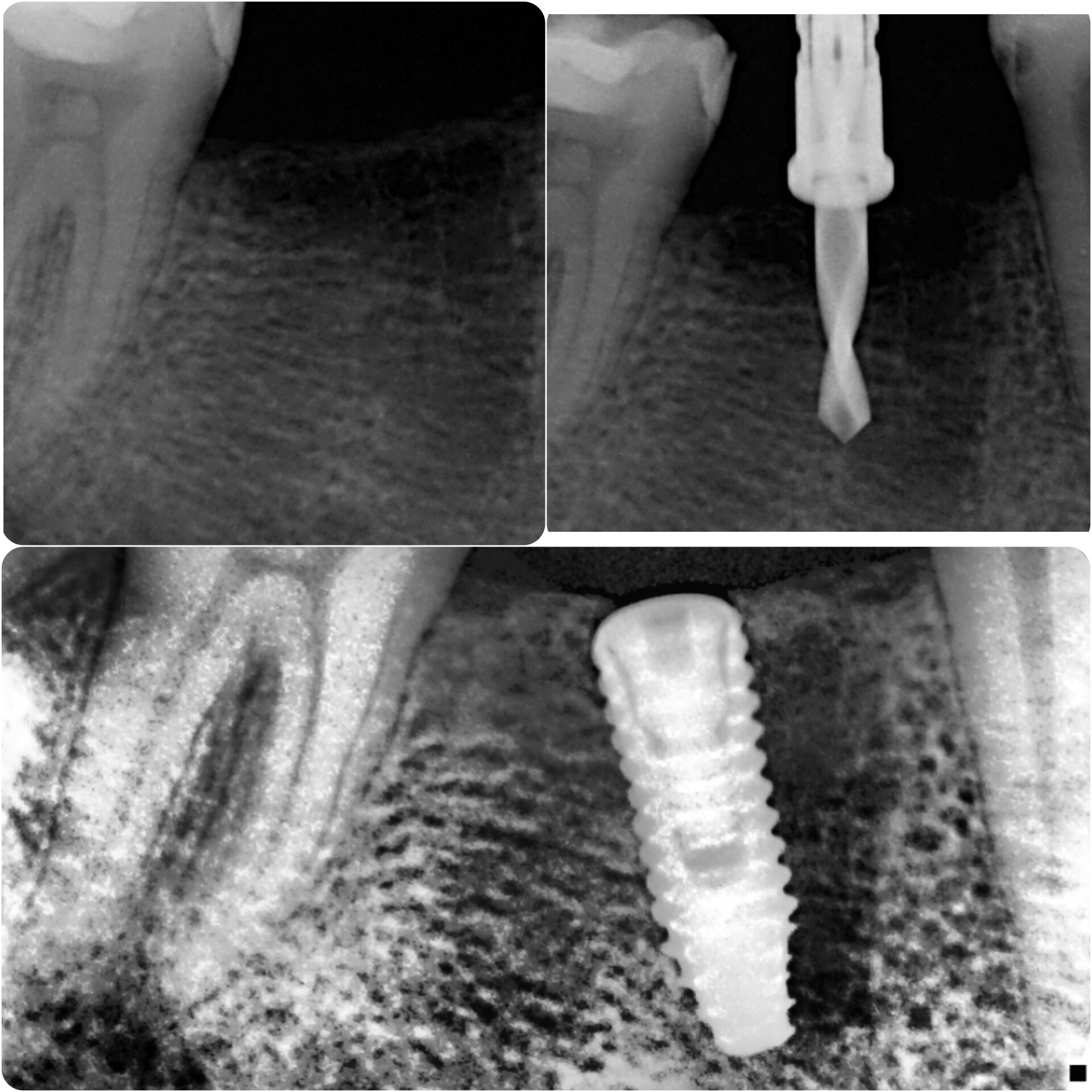
Hello. I am a new practitioner of placing dental implants. Today I have placed 4*11.5 mm Implant in 46 region. Slightly tilted. What will be the consequences of the tilted implant? Kindly guide!
Honestly it will be fine. I would be more concerned about the small diameter and shallow placement but even then it is fine
1 Like
Thank You so much Sir.
This actually brings up another good point in that tapered fixtures can, and do, deviate from the osteotomy by following the path of least resistance. If you look at your check film with the twist drill in place it is not the same angle as the final fixture. I assume this is because the final fixture is a tapered wedge placed into a parallel hole and it will deviate based on bone density to follow the path of least resistance. This is why I have gotten away from using fixtures with extremely tapered apical portions in favor of less tapered and often parallel walled fixtures, I use ZimVie TSV and Blue Sky Bio One Stage. The final placement actually better mirrors the long axis of the premolar and is in a perfectly acceptable orientation but I think the fixture design is what led to this variation. Nice job and it will be fine!!!
2 Likes
Agree with Dr. Scotty… Besides, most of iMPLANT bRANCHES HAVE Angulated abutments to correct them. Now, I’m trying to use only GUIDED SYSTEMS to avoid such problems… I use COWELLMEDI… No problems at all, so far…
2 Likes
it is kinda strange when your pilot drill was very straight but your implant became tilted. I am assuming you used a 4mm implant to replace a molar because buccal/lingual dimensions is narrow? usually if alveolar ridge wide enough for molars i try to use 5mm implants. because platform is wider less chance to flower (platform splitting) under masticating forces. Secondly if your torque is over 35Ncm at an edentulous site. it would save chair time and avoid 2nd stage to place a healing collar instead of healing cap.
the consequence of your distally tilted implant is your crown emergency profile will not be ideal. specially if screw retained. buccal/lingually tilted implants will not have a problem. but distally/mesial tilted implant the path of insertion of the crown is blocked by adjacent crowns. but maybe your lab tech can make it look perfect. good luck.
1 Like
Actually it is not strange at all… Look at the image and you can see the outline of the roots from the previous extraction. The osteotomy was initially drilled down the center to, I assume, engage the septal bone. The mesial root appears less dense than the septal bone and once the tapered apex of the fixture reached thie apical 1/3 of the osteotomy it just followed the path of least resistance right into the softer mesial bone. You can actually see on the final film where the tapered end of the fixture tracked perfectly along the cortex of what was the distal aspect of the mesial root causing it to fall into the softer bone of the mesial root space. The degree to which this fixture deviated from the initial hole matches perfectly the degree of taper at the apex of the fixture. I was a hobby craftsman long before I was a dentist so this type of carpenter work just speaks my language…
1 Like
but you do see the drill the dr is using? looks like there’s a sleeve or is it a guide? like a keyless surgical stent?
1 Like
It’s not surgical guide, it’s a drill stopper so that I can’t go beyond the pre determined length! Here I am using DIO implant n surgical kit.
So I assume you drilled your pilot to a predetermined length short of your final depth and took the film to check the position. Since it looked good then you completed your drilling sequence to depth and then inserted the fixture. Because the fixture has a tapered apex it contacted the more dense cortical bone on the distal aspect of the mesial root and the resistance caused it to divert into the less dense space of the mesial root. I first observed this sometime around 2007 when placing a Nobel Biocare Replace into a similar site. I concluded that the tapered apex along with the “soft” thread pitch of the fixture facilitated this deviation and that was my first indication that one size fits all does not apply to implant dentistry so I started looking into less tapered fixtures. It happens all the time in my shop when a wood screw contacts a knot or a dense area so it makes sense to me that the same thing would occur when doing carpentry in the mouth…
1 Like
Thank you Sir for this beautiful and detailed explanation. I think this was reason for that implant deviation! So which brand of Implants do you prefer for your regular practice?
Anything with gradual taper like a Zimmer TSV or parallel walled fixtures, Straumann or BSB One Stage, have worked well for me. I also drive a Ford F-150 when I know good and well that Chevy and Dodge make good trucks but I prefer the ride of a Ford. I think most of the fixtures manufactured today are designed for maximum initial stability and thus have too much taper but that is my opinion as I have come full circle back to using some of the classic designs… Not because they are state of the art or inexpensive but because they work!