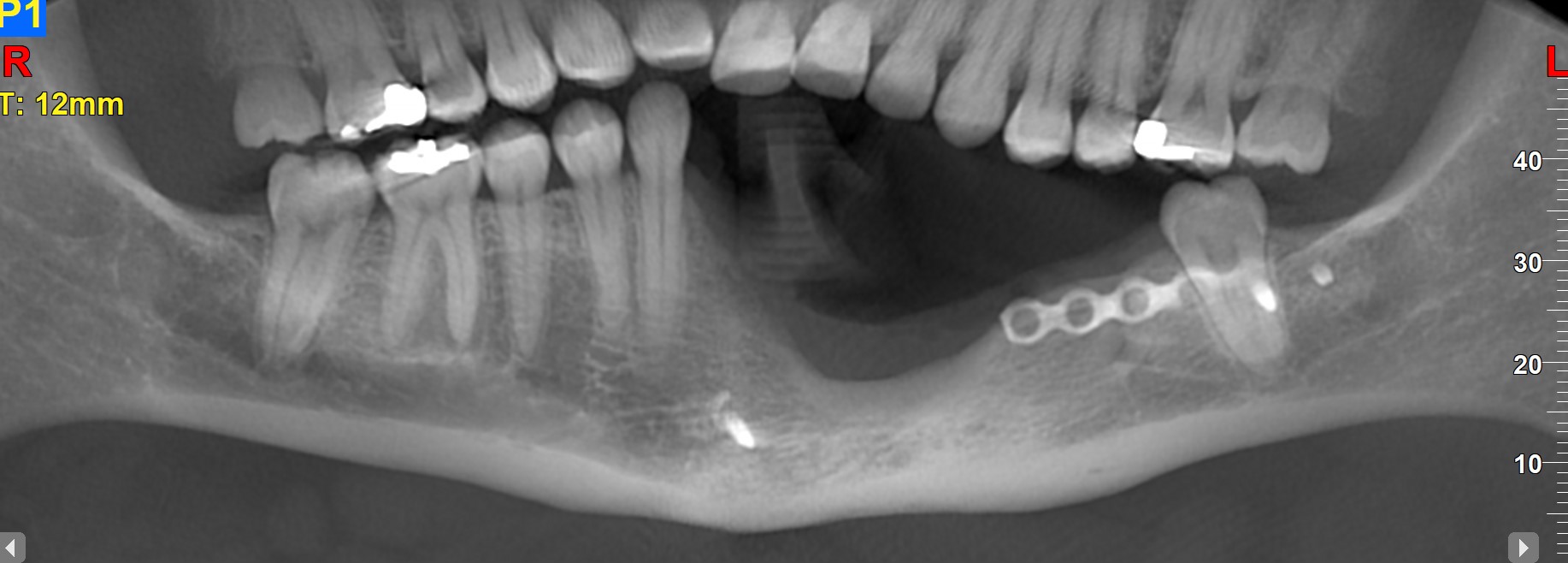
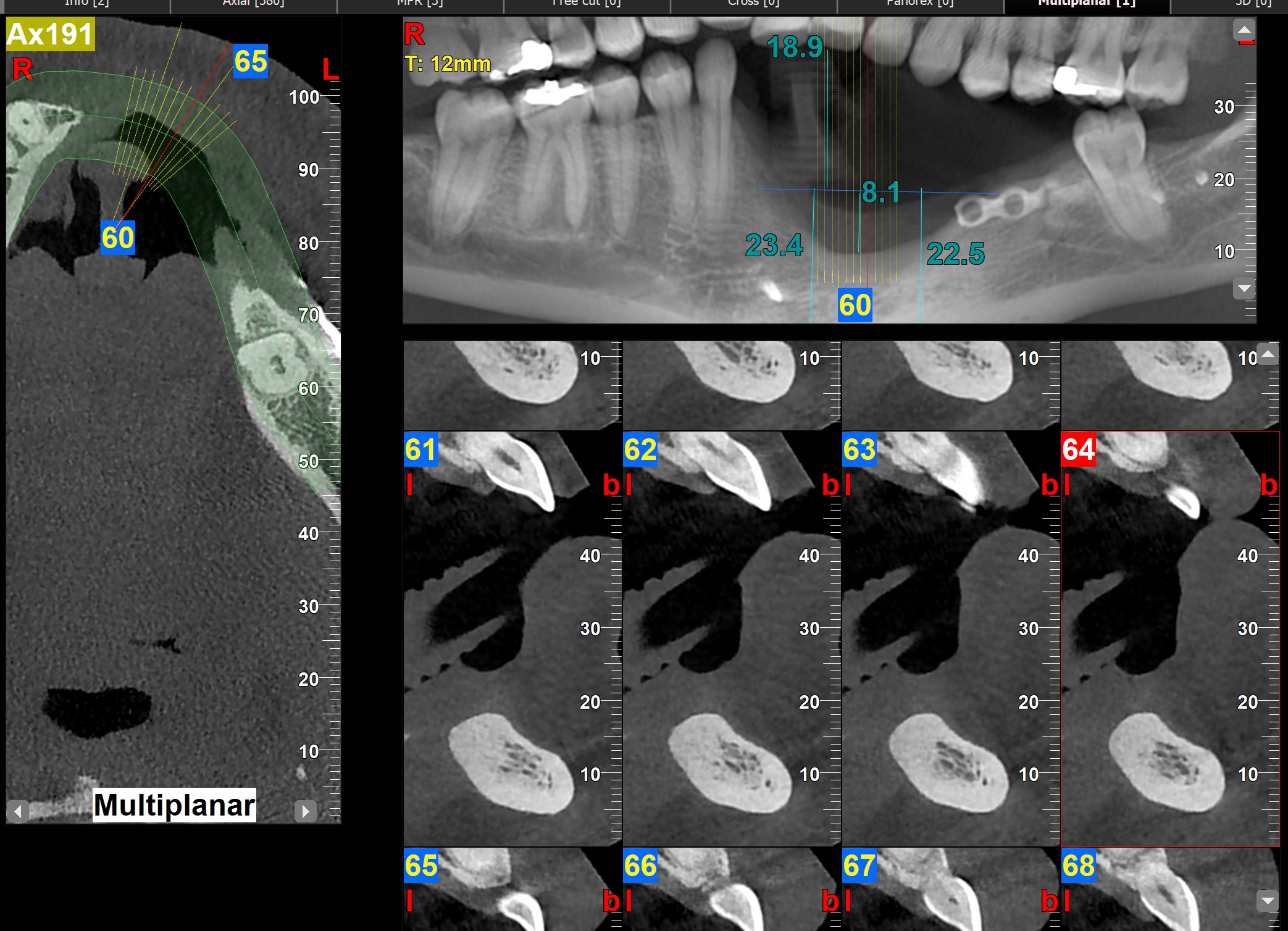
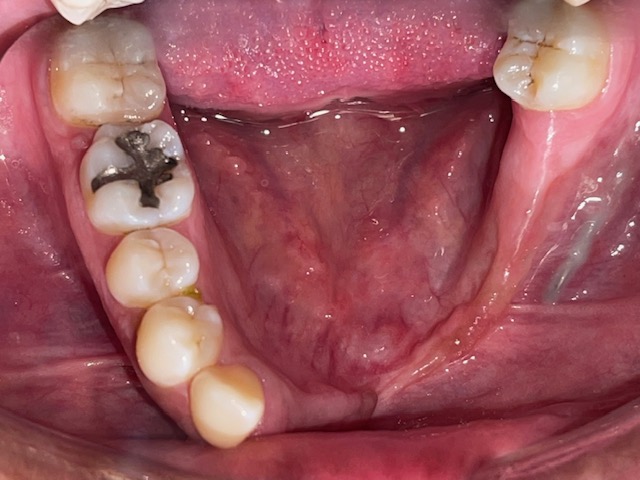
Here is a challenging case. Female pt 28yo. h/o ameloblastomax2 10 years ago. no other comorbidities. no recurrence since 10 years ago. Reports currently using an ill-fitting PLD which she forgot to bring at consultation and dont use that much. She has seen many GP and specialists and no one willing to tackles this case and have referred her out. which i understand why. This has become my challenge and perhaps a case presentation for the future. I already have a plan for her which involves GBR w/ BMP before AOX. what you guys think? will update next year.
By AOX are you planning to extract all of her remaining lower teeth? I would consider 2-3 implants to support a bar with a clip on obturator style prosthesis and preserve her remaining functional dentition. I doubt that she doesn’t were her prosthesis simply because it is removable but rather because it is an ill fitting tooth-born prosthesis which was likely made a long time ago. An AOX can always be done later but it seems pretty aggressive to remove her teeth now, at only 28 years old…
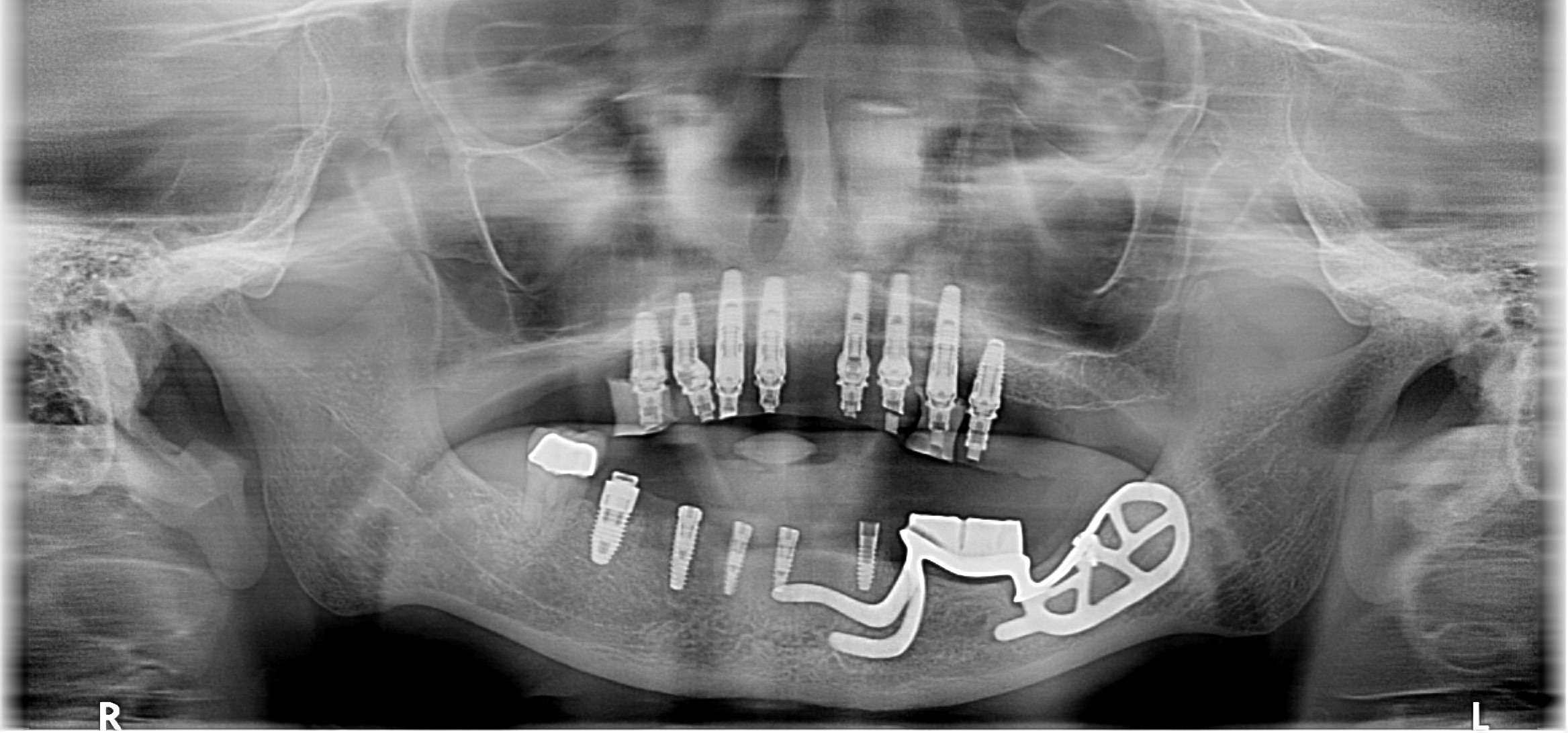
I inherited this case and was only responsible for placing the 3 implants in the 25,27, and 29 areas as everything else was already installed when I saw her and we converted her to a full lower AOX. The subperiostial cage supports a bar with a removable clip on portion and it actually works really well. This image is from 2018 but I see her 1x each year and can attest to the satisfactory results from this clip on section which I think might serve your patient well, on traditional fixtures rather than a cage.
she does not want anything removable. so it has to be fixed. either restore the section of teeth that missing or replace whole lower arch. replacing whole lower arch may seem excessive but i think functional, aesthetics, replacing whole arch would be best for the long term. also im confident the AOX implants would last her a life time. but the prosthesis would probably be changed every 20 years. i just hope i will be there to help her replace the prosthesis when it’s worn down.
i dont let patient dictate my treatment plan. just like the patient in your pano. 8 implants on max is kinda excessive (i know its not you). restoring lower arch with mickey mousing and mixing implant fixed and removable may work but just not an ideal or optimal treatment. plus why retain that 31? but you also converted her to an lower AOX. in your patients case AOX is definitely the best option.
i hate to repeatedly fix patient for the same problem only bc you compromise treatment plan with patient’s request or desire. sometimes they just dont have a choice. i rather refer the patient to some other dr to struggle. its not worth my chair time. sometimes it’s my way or the highway.
Makes sense… I assume with your confidence in the longevity of the implant treatment that you provide that you must have been doing this for 30+ years. I am only 25 years into my profession and I don’t yet have the confidence to slick a 28 y/o and promise them a lifetime of success with a treatment modality that has only been widely used for 10 years. I admire your confidence!
lol dr scotty. so sarcastic. you are definitely more ancient than me. im a young buck (perhaps that’s why i have less fear). Full arch implant supported prosthesis have been around for a long time. almost since the birth of dental implants in mid 60s. i am sure you’ve seen some blade implants. Althought AOX has been more popular for the past 20 years. i am sure its been around for at least 40yrs. just the patients often expire before prosthesis/implant failure. of course I have confidence in my treatment. so do you, since you’re still placing implants and restoring them.
i did give her 2 treatment options. but just only restoring #19-26 will also have problems or revisions in the future, alas we still have to consider AOX. i rather place implants one time and replace prosthesis than replacing everything in the distant future.
Besides, im not confident to grow >1.5cm of bone vertically even w/ BMP. but 5-8mm vertical augmentation seems tangible.