


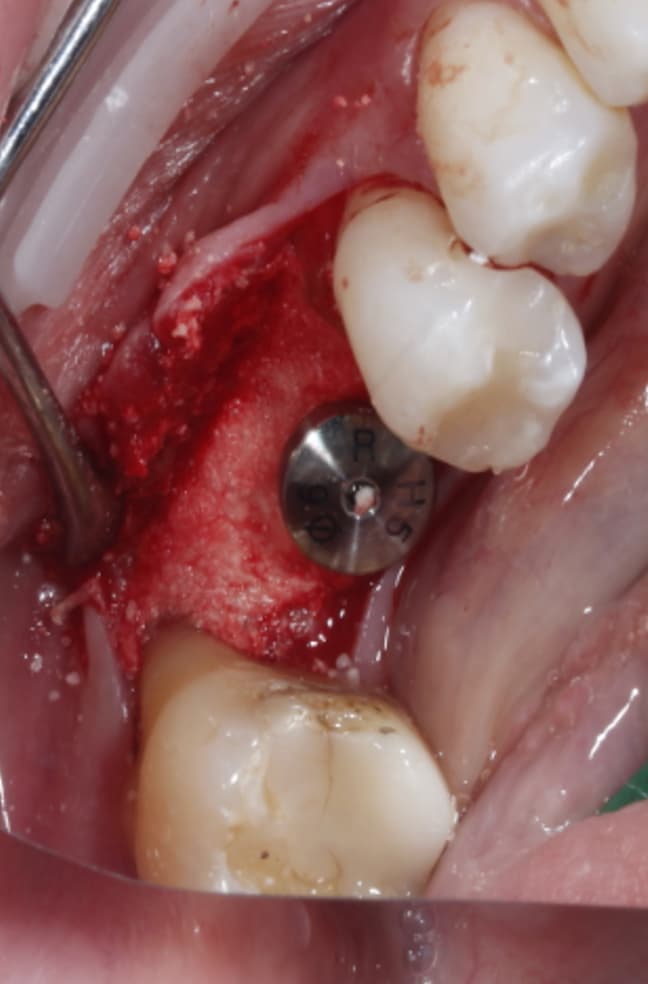
at the end, Ethoss, beta-TCP was grafted and moulded around the implant to close again.
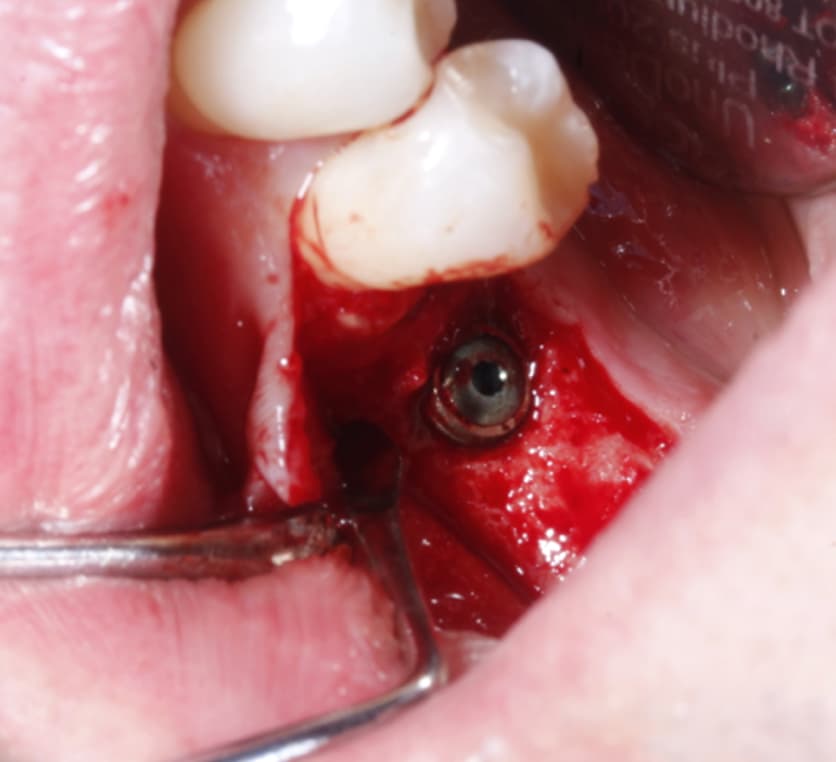
could anyone explain how this buccal wall disappear after implant placement?
at the end, Ethoss, beta-TCP was grafted and moulded around the implant to close again.
could anyone explain how this buccal wall disappear after implant placement?
Ossification is a complex and sometimes unpredictable process. I think 10 weeks is a too soon for implant placement since the extraction socket hasn’t fully calcified and you still have spongy bone inside the socket and psuedoperiosteum on the occlusal of the socket. I noticed radiographically i can see still see the socket. I usually enter and place implant at 4 months minimum post extraction, ideally 6 months, when radiographically the socket is mostly radiopaque indicating more calcification and ridge remodeled consistent to final dimensions.
I also noticed at implant placement i see 2 occlusal defects mesial and distal of the implant (most likely indicating mesial and distal root of previously extraction). which indicated the ridge is not fully ossified or calcified. i wonder if during osteotomy you felt soft bone instead of the usually hard mandibular bone. i think at implant placement you should have grafted. the occlusal is kind of flat, as if you did some occlusal reduction of some kind.
your buccal flap is also too deep which exposed the buccal plate and cause further resorption. at edentulous sites i usually only flap occlusal and stop at the buccal occlusal line angle of the ridge. avoiding exposing buccal plate to avoid devascularizing the buccal plate. every time you flap you will lose minimum of 0.5-1mm of bone. that’s research proven by perio.
some of my OMS friends don’t even flap these days. they just drill through the gingiva and place implant.
Your implant position is impeccable. good depth and orientation in the ridge.
this is my take on it. hope it helps.
I think it is just coincidental bad luck… If you place 100 implants under ideal circumstances then statistically 3-4 of them will fail. I agree with everything Teng has said except that I have been routinely placing fixtures at 6-8 weeks post extraction for the past 20 years and I do it because I want to place the implant while the extraction is still soft and spongy. I feel like waiting 4-6 months is fine but my understanding of the wound healing process would suggest a benefit in wounding the site via an osteotomy and fixture at the 6-8 weeks point to sort of jump start the process. I have no proof for this theory other than 20 years of experience and success practicing this way and again I think you just experienced a bad luck scenario and I would not suggest changing anything.
On another note I could not even speculate on how often and to what degree this exact scenario might occur in my practice. I say this because I rarely, like less than 1% of the time, place an implant without attaching a healing abutment at the time of surgery so I don’t uncover and take a peek at too many fixtures as long as they ping when tapped on after 12 weeks. Different philosophy of practice but having been trained on tissue level fixtures which are designed for one stage healing I have never been a fan of two stage implant protocols unless necessary for a temporary prosthesis. This could be a more common pseudo-problem than I am aware of… Nice job and thank you for sharing this… I do believe that the current trend of installing aggressive threads on implant fixtures is potentially problematic and might contribute to more of this necrosis type of bone resorption. If this does occur and I am just not seeing it because I hardly ever need to uncover a fixture it has never presented a problem or perhaps it doesn’t occur because I still use Straumann TL and Zimmer TSV which are old school fixtures with boring soft thread designs???
I just had similar complication. sometimes just have to think of it as “shit” happened. I dont have explaination either.
i placed implant at edentulous site #28 and immediate #29 during extraction of #29 root.
healing was uneventful. but at 4 months you can see PARL at mid implant #28.
i did similar procedure, same time, same implant, yet #28 failed. (#30 had to removed later due to pain, failed RCT)
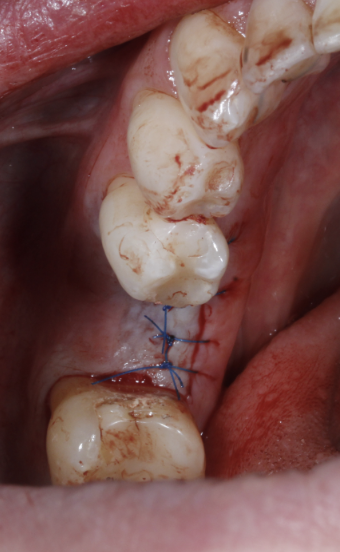
i removed implant and removed PARL and did a flap to take a photo of the defect. doesn’t even make sense to me. edentulous site should be a slam dunk case. but somehow #28 had a sinus tract and PARL. I grafted it and will wait for 6 months before placing implant.
like dr scotty says. sometimes just coincidental bad luck even if you did everything correct.
Just out of curiosity what was the estimated insertion torque on the #28 fixture. I ask this question not because I believe in insertion torque as an indicator of future success but because I assume it was placed at high torque which is extremely common in the lower premolar area. I have experienced far more failures and head scratchers with straight forward fixtures inserted at high torque than I have fixtures placed at low torque, <30Ncm… And I place healing abutments on all of them, even the so called spinners, so long as they don’t wobble in the osteotomy.
usually i torque implants to 35Ncm, occasionally at most 50Ncm. I’m pretty anal about this actually. similar to you. i observed more failures at high torque than low torque. Spinners i leave for 6 months and magically they integrate perfectly. If there’s any implant failures, implants usually get infected and exfoliate. I usually take a PA at 1 month post placement. if everything looks good. i wait another 2-3 months to take impression. then deliver a crown 1 month after. If there’s any radiolucency. i either wait a month to see if it resolve w/ PO ABX or remove the implant, especially if i see a sinus tract.
i use cover screw for immediate placement w/ BG and spinners. Only implants placed in edentulous ridge w/ >35Ncm torque i use healing abutments. Just me being conservative. I observed if i place a healing abutment on immediate implants w/ BG, there’s a tendency not to get a good bone fill around the implant platform.
Fair enough… I certainly wouldn’t suggest changing what works!
upon hindsight it probably because i used ‘ slow speed osteotomy: osteotomy of 300rpm without any water’ that probably was the reason. i used to do 800rpm with water but the mentor suggested slow down to have better tactile sensation.
is ‘ spinner implant’ same as implant without primary stability ?
correct, a spinner is when you can rotate the implant with your fingers in the osteotomy,
i always irrigated whether slow or fast, unless im using versah drills and propelling BG into the sinus.
but like dr scotty says, i doubt thats the reason for resorption. most likely just “bad” happened. beyond your control.
For about 4-5 years I drilled every osteotomy at 250 RPM with no irrigation. I switched about 15 years ago to 750 RPM with irrigation and the truth is I have noticed zero difference. I will continue to use 750 RPM with irrigation not because of any difference in outcomes but because it is just more widely accepted within the industry and its easier to defend in case of a problem. I doubt that your low RPM without any irrigation is a factor in this case but you are probably wise to go faster and wetter because not too many folks out there will show us grace doing it dry…
Assuming that “we” irrigate during an osteotomy as a way to cool the bone and prevent overheating isn’t it odd that very few people irrigate while inserting the implant. I have done a lot of carpenter work over the years and its amazing just how much heat is generated by a threaded screw inserted in wood. I can only assume that torquing a wide implant into the bone would generate a lot of heat too… most likely more heat is generated by inserting the fixture than when drilling with sharp tools regardless of the speed and/or amount of irrigation. I think we should be more concerned about irrigating during placement but that is above my pay grade.
im surprised perio has not published a paper on heat generated during implant insertion. i irrigate during drilling to wash away debris. sometimes i accidentally irrigated during implant insertion. i accidently stepped on irrigation pedal when switching modes ( i have big feet). i don’t know if it makes a difference in cooling the bone during insertion but it was harder to see how deep i place the implant due to water refractory effects.
i know our profession sometimes is plagued by anecdotes. passed from faulty to students, dentist to assistants/office managers, dentist to dentist, etc. and if you don’t follow the masses, you might be labeled a dangerous or reckless dentist. Even now when new research and guidelines should have changed the way we practice, lots of dentist still follow outdated teachings blindly without adapting to new information.
IMHO it does cool the bone if we irrigate during insertion but I doubt if it makes much of a difference since the vast majority of fixtures are inserted dry. For tactile sense and optimal vision I think it is best to use high quality sharp drills at slow speed with no water to block our view while drilling the osteotomy as well. Another advantage of drilling without irrigation is the increased volume of autogenous particles that can be harvested from the flutes of the drill. This is of course only my opinion based on experience and even though I think it is fine to do this I still irrigate during drilling and placement just to satisfy the skeptics and feel comfortable that I have taken all of the unnecessary steps to comply.
another question dr scotty. do you see more failures with implants buried w/ a cover screw or implants with a healing abutment?
Personally I have seen a higher percentage fail when buried with a cover screw which is why I rarely submerge an implant. I place a healing abutment on bone level fixtures at the time of placement 99% of the time now and my go to in the posterior is a tissue level fixture so my sample size for buried implants is pretty small in comparison.



