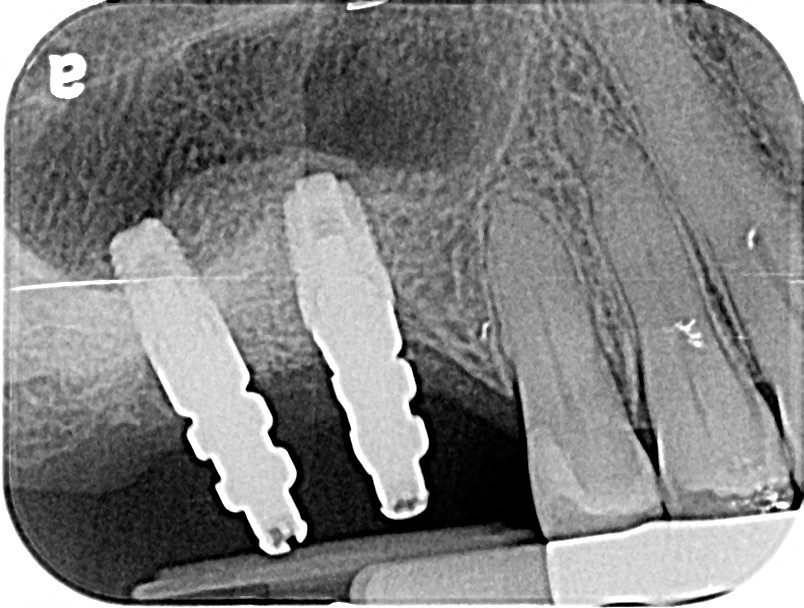
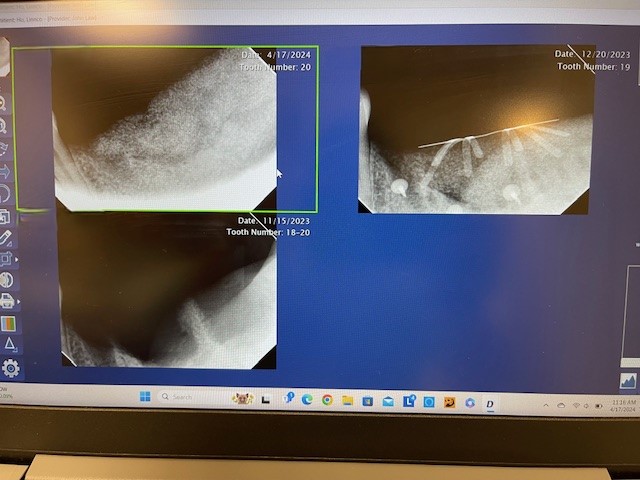
I had trouble seating this 2 unit fixed zirconia screw retained bridge today. My periodontist requested the bridge be splinted to reduce any chance of future bone loss. They are Neoss 4.0x7 and 4.5x7. I could remove the bridge from the lab model with my driver but could not seat in the mouth. I checked the mesial contact of #3 and it was passive. I am not sure how to proceed as this has never happened before. I know the implants are deep. Should they be separated and made as individual units? Should they be made cement retained? Please help. I have attached xrays of the impression posts and the bridge in place.
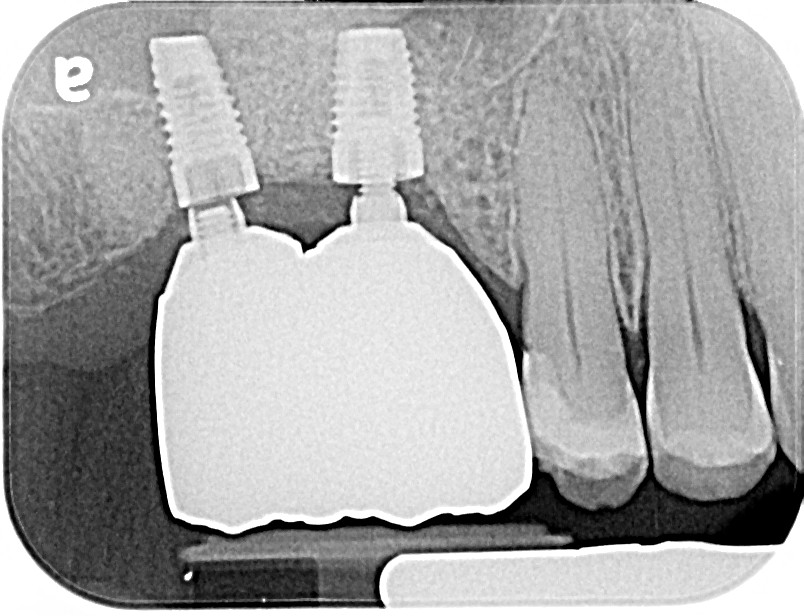
Great x-rays. I would guess that since the implants are not parallel that the splinted teeth, as manufactured, will never seat. One solution could be to make 2 individual custom abutments and cement splinted crowns to them.
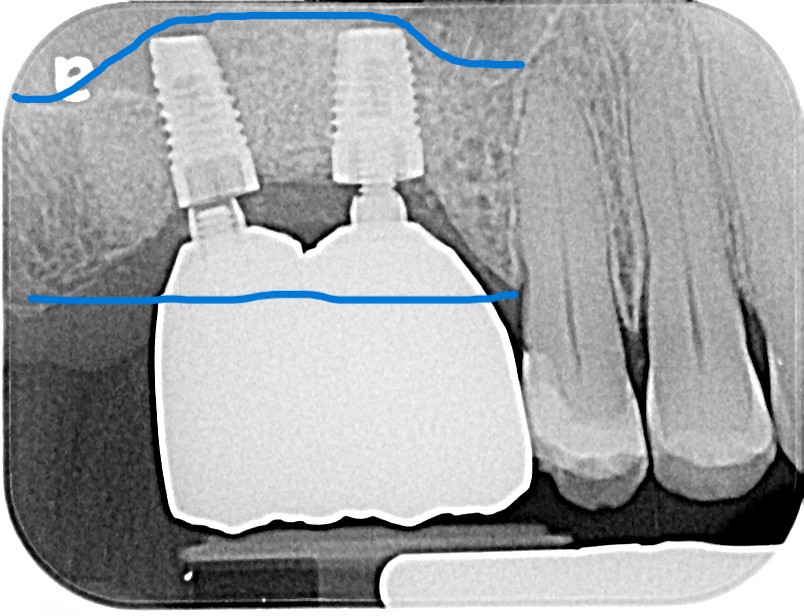
You have enough crown height, bone & gum tissue. I would select an appropriate Multi unit abutment on each and make seperate or joint screw reatained crowns ![]()
Hi;
It looks like the problem is on the mesial aspect of the bridge that is almost touching the bone, and was probably bleaching the gum when you were trying to seat it.
There was probably a problem with the impression or the model.
You should retake an accurate impression (preferably open tray), and send it to the lab along with the bridge and let the lab make the corrections.
Let me know.
2 Likes
I suspect it was an error with your impression taking .
Try redoing it, making 2 separate screw retained crowns and don’t lose any sleep about any potential future bone loss.
2 separate crowns are easier to maintain and retrievable if necessary
I would assume that the goal was to splint them via a one piece cement retained prosthesis on two individual abutments as the likelihood of fully seating a screw retained prosthesis with engaging abutments is impossible. If you are of the camp where cement retained implant fixtures are bad then I would suggest using multi unit abutments and attaching to those but I would cement on custom milled individual abutments.
A better topic of discussion is how/why would splinting these prevent any future bone loss. I would be more inclined to expect more loss with a splinted case due to compromised hygiene and the resulting food trap…
There is a new study that was published says that, splinted crowns ( Implant -abutment ) has fewer mechanical complications than Individualized or non splinted crowns, with no significant difference in biological complications ( for hygiene reasons ) .
Interesting. Can you post the reference to the study or a link? Thanks.
Please post that study as my 2 decades of experience would suggest quite the opposite…
Except that a single complication with any portion of a splinted restoration is a potential complete failure while a single complication with an individual unit is a single complication with an individual unit…
Hope this link works.
Thank you. Unfortunately it does not address the degree to which a complication on a splinted restoration significantly compounds the problem. A mechanical complication on a single unit is a simple mechanical complication while a mechanical complication on a splinted restoration is a catastrophic failure…potentially. I think it is also important to consider the type and/or brand of fixtures being restored and/or splinted. Many of the lower cost knock off products (Implant Direct, Neodent etc…) are not manufactured with the same degree of precision and their connections, while interchangeable with the higher quality products, are more prone to complications. I think it is unfair to lump different products of vastly different quality into one category and make such a general statement. I say this as someone with a background as a machinist/mechanic. Quality and tolerance makes a huge difference IMHO.
I believe that the lower cost/lower quality and precision fixtures likely do benefit from being splinted as it minimizes the slop in each individual connection. With a higher quality and more precise connection (ZimmVie, Straumann, 3i) type fixture mechanical failures are virtually eliminated due to the precision of the craftsmanship. This is assuming that OEM components are used. In today’s mixed bag of implant practices it is difficult, if not impossible, to compare mechanical failure rates as we have no way of accounting for generic components.
your periodontist should be better at augmenting bone. augmenting the vertical defect in conjunction with sinus lift would have made implant placement and selection more ideal.
Anyway, most likely you would need to use individual implant crowns.
What do you mean by “augmenting the vertical in conjunction with the sinus lift”. I was under the impression that a sinus floor augmentation was vertical augmentation and how would more vertical change the nature of the issue in this case.
Thank You
vertical ridge augmentation coronally.
Sinus lift add bone apically. im talking about growing bone coronally.
it wouldn’t change the current problem because the implants already placed and integrated. but implants would have been placed more ideally if the correct alveolar ridge is achieved before implant placement.
Thank You. Since you point this out I assume that you have experience and a “predictable” technique to achieve this seemingly ambitious goal. Would you mind sharing your technique as I would not consider this to be a reasonable and/or predictable expectation.
i learned from Istvan Urban. His sausage technique is by far the simplest and user-friendly technique to achieve vertical and horizontal augmentation. i have done many cases. mostly horizontal. a few verticals. this max posterior isn’t too difficult. plenty of tissue to achieve passive closure and aesthetics is not an issue
I have yet to use BMP. I do have a cleft palate patient i would like to try BMP on a cleft patient. Im restoring her posteriors before she feels confident enough for me to restore the cleft. the photos belongs to another pt.

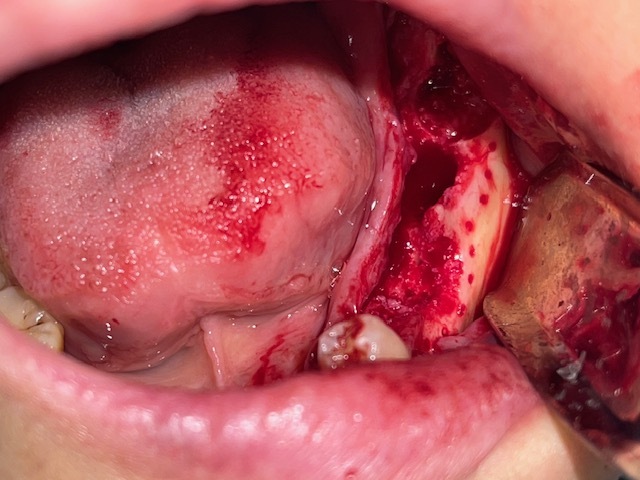


I agree w/ you scotty. among all dentoalveolar surgery. i think ridge augmentation is by far the most challenging and most difficult to achieve consistent results. but also the most rewarding.