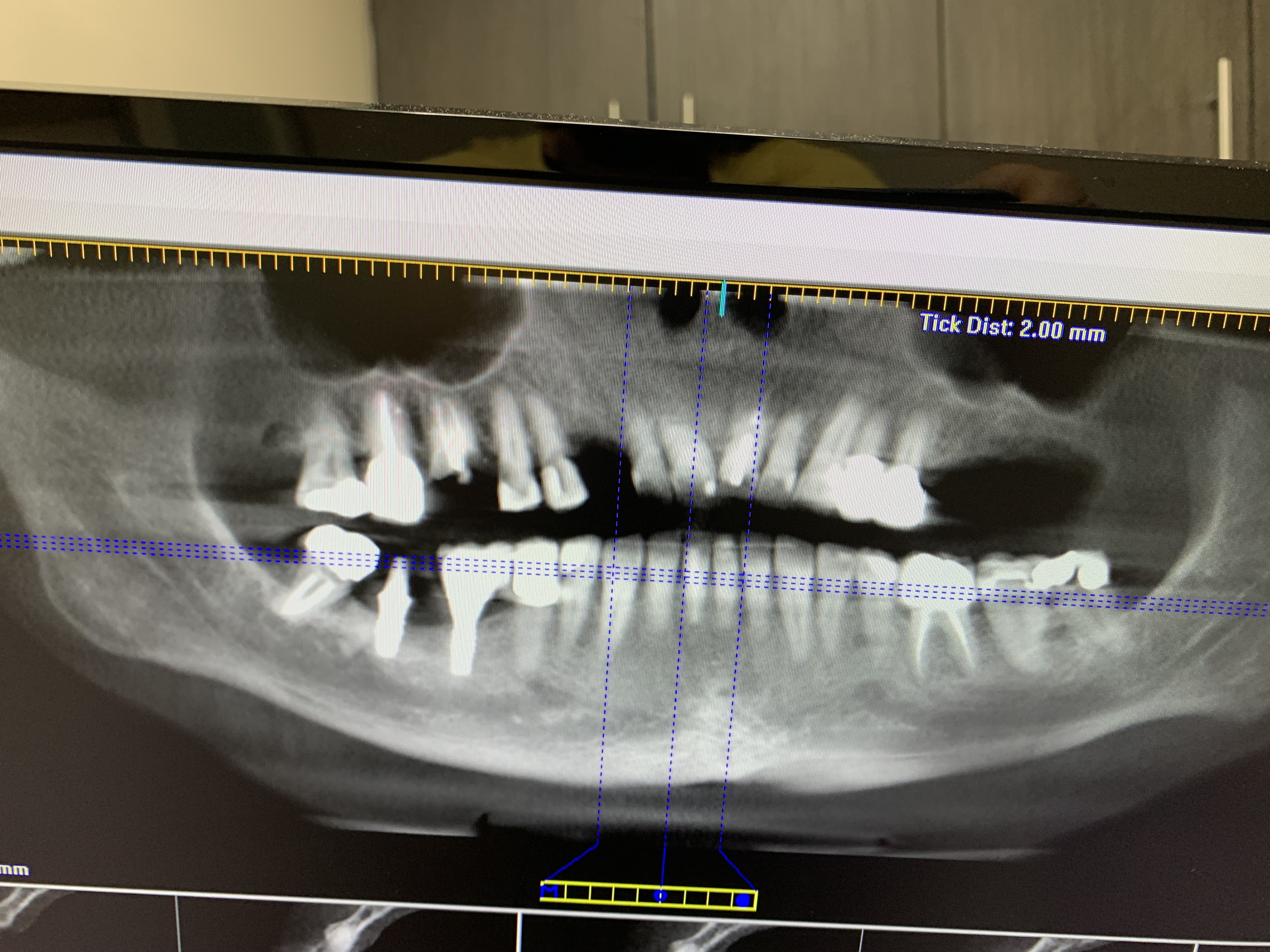
Surgeon was initially supposed to place an implant upon extracting the tooth. However, instead he extracted the tooth (Canine) and bone graft was done. At the 6 month post extraction and grafting visit, surgeon says the bone is too thin for an implant. He is seeking consult, suggesting stretching/augmenting or adding bone from different area or extracting #5 and placing narrower implants. The initial scan prior to extraction demonstrated a similar finding. He claims he was aware of it but chose to wait and see results of the initial graft. Would appreciate any suggestions.
Guest comments:
Just reading the question, and without even looking at the attached x-ray, I would say that your surgeon has done everything anyone reasonable surgeon would do, and I would do as he/she says: Get a consult and explore these additional options. Very few surgeons would place an immediate implant in thin bone. Grafting and waiting is the better option, in my opinion. Now that you have done that and the surgeon is still concerned with the thin bone, then yes, you will need to seek another consult to determine the best course of action.DeeR GeeSin comments:
what am i missing here? The bone graft failed or it was inadequate. The bone shouldnt be too thin-he bone grafted the area. whats there to consult? the pt needs bone grafting, not having another tooth extracted. whoever is responsible, between the surgeon and the patient needs to pay.Guest comments:
"What am I missing?" Firstly, bone grafts do fail. That's nobody's fault 99% of the time. Either you graft again or discuss other options. Second, I think the question was actually why they didn't do an immediate. And I think the answer is that an immediate was not appropriate given the bone.guest . comments:
If graft's done properly, shouldn't failed. I would go ahead and do both immediate and bone graft same day appointment.Guest comments:
Utter nonsense. Grafts fail. Immediate is a terrible suggestion. See Matt Helm above. He is correct.guest . comments:
yup nonsense! can't seem to add your input so you recommend someone else'?Guest comments:
Responsible for what? There is no guarantee. Such an annoying responseDeeR GeeSin comments:
youve never had a patient ruin a bone graft procedure? where did i mention anything about guarantees? youre annoying.Peter Hunt comments:
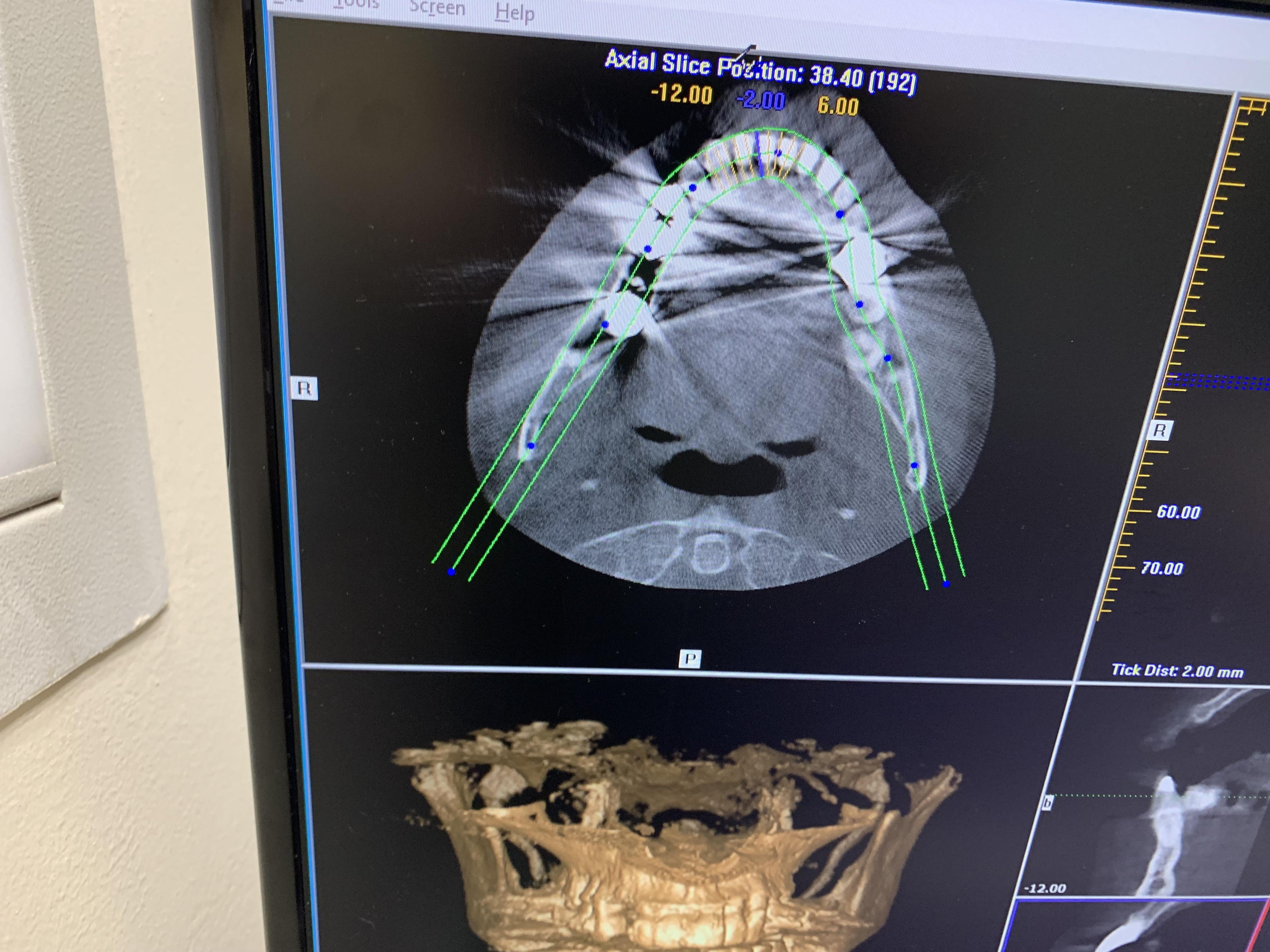
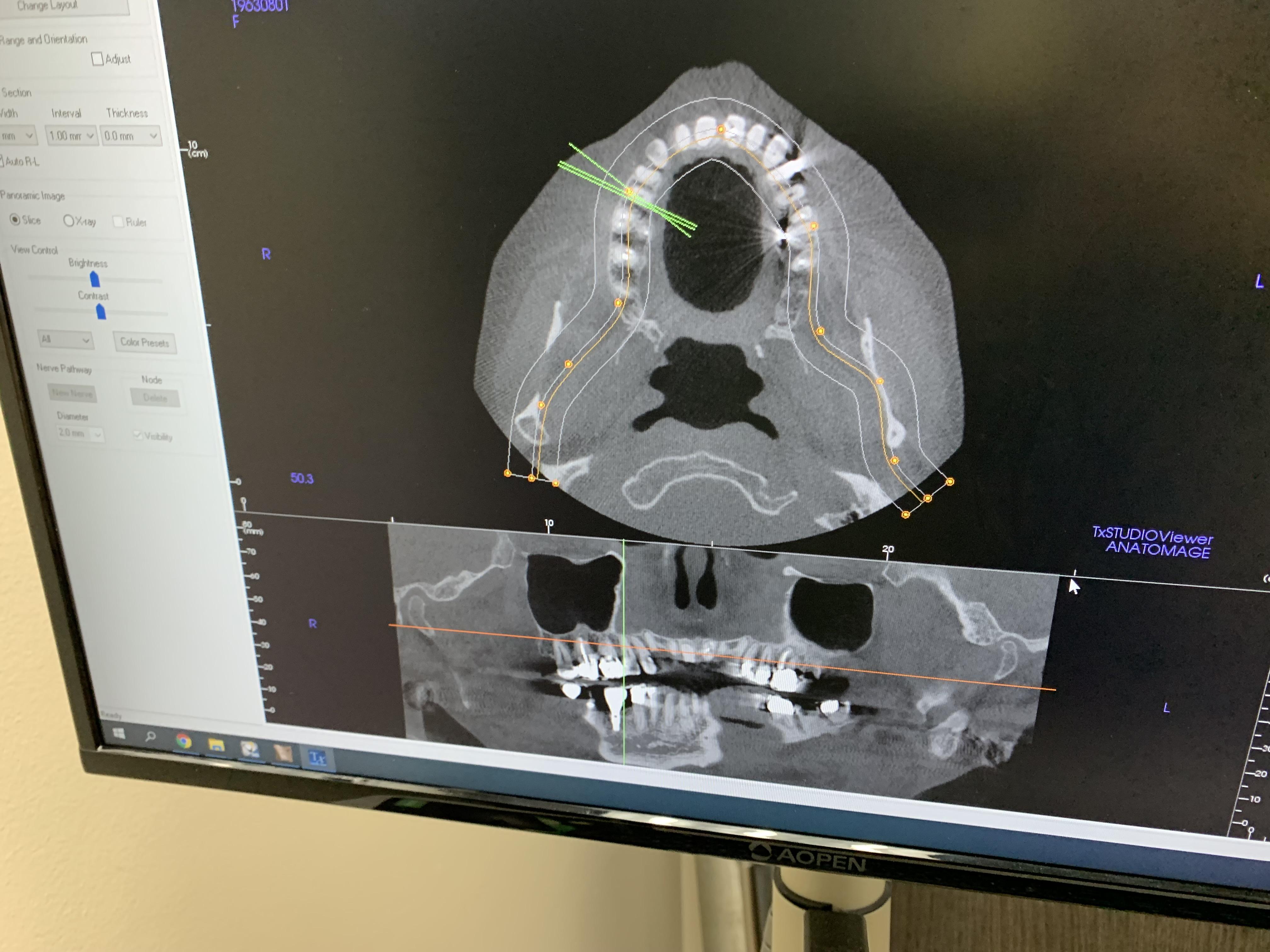
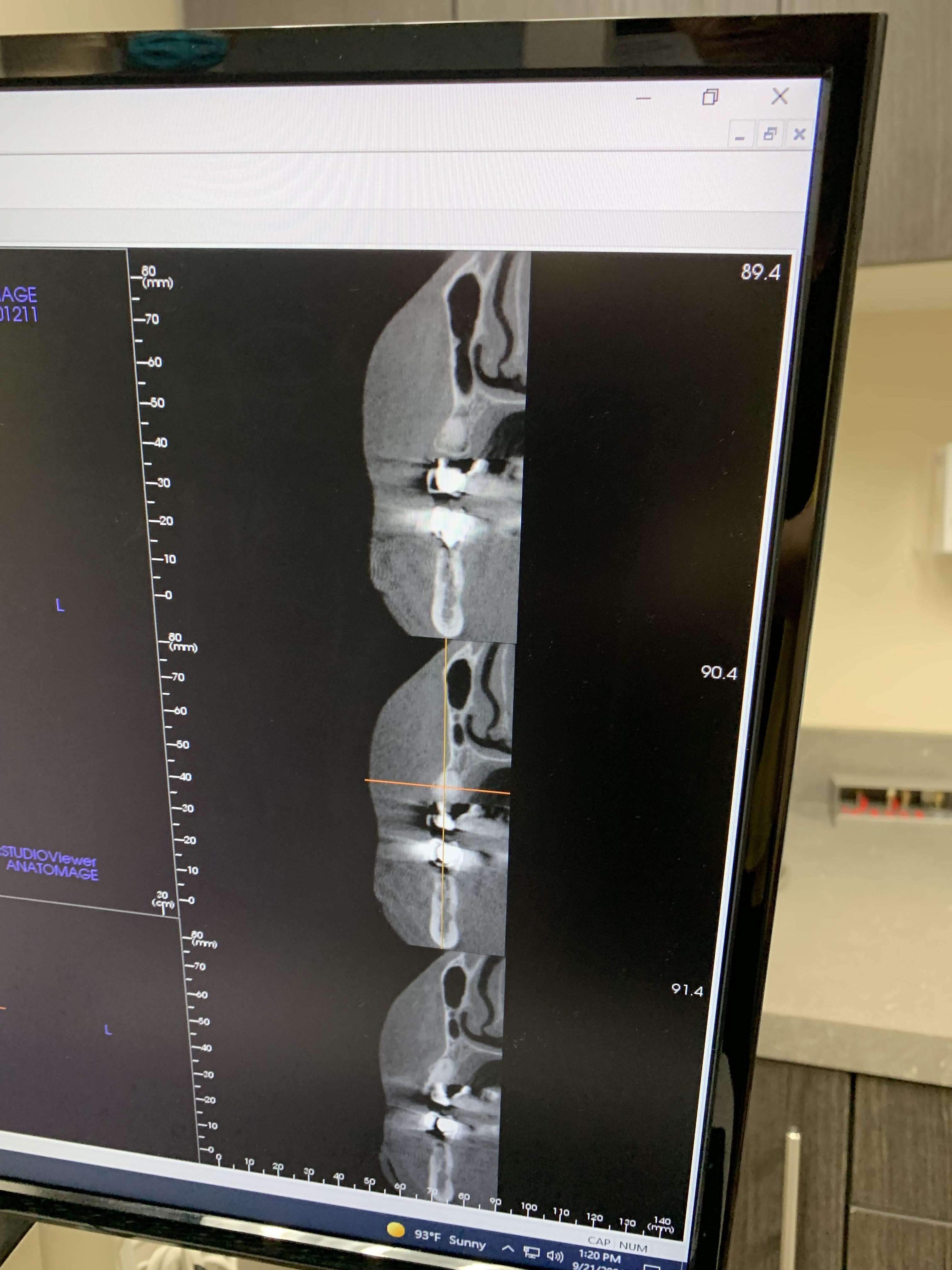
It would be very helpful here to see a cross-sectional view of the region of concern, preferably with a proposed implant super-imposed. Without this, we are left guessing as to what the situation really is.Yaşar Çınar comments:
Bicortical techniq with narrow implant.Matt Helm DDS comments:
You should have included the CBCT slices of the area in question. However, if the OS says the bone is too thin, he's probably right. He didn't to the immediate placement because bone was insufficient at the time of extraction. Surgeons rarely, if ever, take outsized risks. However, extracting #5 is not the answer! "Back up" a little and see the big picture of the WHOLE case! Considering that both bicuspids and the molar all need reconstruction, a 4 unit mesial cantilever bridge would be more efficient, more expedient, and definitely serve the patient's interests better. rather than putting him/her through additional surgery which will take months and may, or may not, ultimately yield the desired result.Guest comments:
Without a preop film or cbct just spitballing here. When I don’t get a great result and have to regraft at time of implant placement I’ll use Versah burrs and PRGF with the bone. Implant itself helps keep the bone expanded. Would have to know how much width needed vs a block graft. The anterior teeth need to be considered in a prosthetic plan a lot of vertical bone loss, difficult to do these piecemeal.Greg Kammeyer, DDS, MS comments:
I didn't hear in your description that the #5 needed to be removed. Yes, bone grafts fail or more often, we get less bone than we wanted. Confirm if the patient is on SSRI's, PPI's, diabetic, smokers/nicotine users, bisphoosphonates, and if they exercise. All affect bone healing. Certainly this isn't the OMS first disappointing graft. Clearly he/she has other grafting choices than a small diameter implant for a cuspid! GBR with bone scraping and or growth factors works nicely. THE LAST thing I would consider is splinting a bunch of teeth to cantilever a pontic. Hygiene issues, what happens when that fails?Doctor J comments:
No # 5 was not to be removed. Patient has no medical issues.