In 2020, I had implants placed in teeth 13 and 14. Shortly after they were uncovered, I experienced bone loss around the implants. This was my original question: Bone loss shortly after implants placement?
The implant at tooth 13 failed in 2023. Both implants were extracted, and bone grafting was performed. New implants were placed in March 2024. Immediately after the placement, I experienced pain and discomfort in the sinus area, which lasted for months, even after uncovering, until the temporary crowns were placed. Constant pain in the sinus area after implants placement with an internal sinus lift 4 months ago
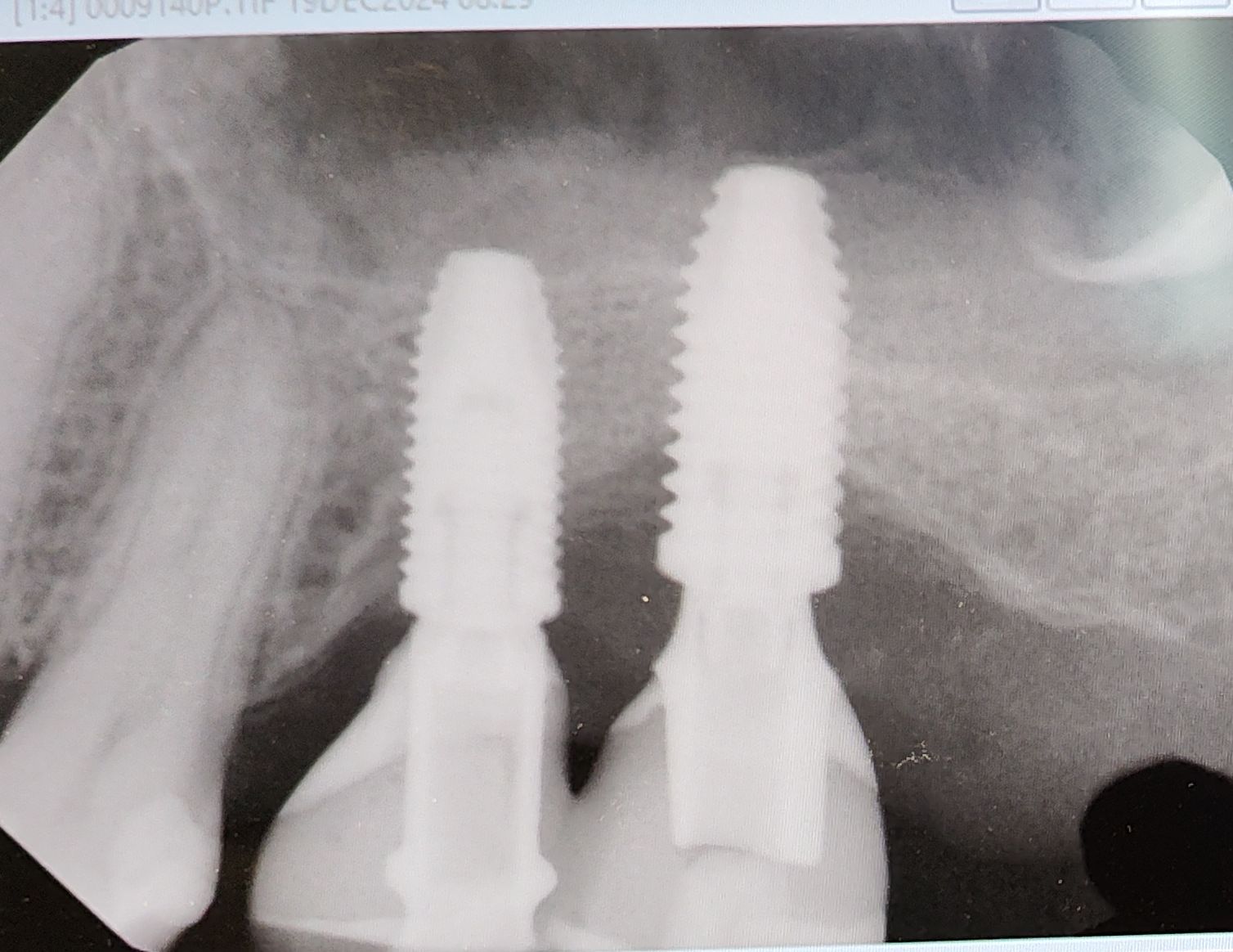
The latest X-ray shows bone loss again, similar to what happened with the previous implants.
Why does this keep happening? Could it be peri-implantitis? I have two other implants that have been successful for many years, but these two fail so quickly. Could it be an issue with this specific area or the surgical technique?
Dear Patient,
This is forum for dentists ONLY, not a place to try and gleen answers from for your own personal situation .
While I undretsand why you want free opinions, you must refrain from using this forum for your own personal gain.The best place for you to get answers from are the dentists that you are currently working with. Best of luck
I have been practicing implant dentistry since 1994 and have seen numerous cases of bone loss around implants that did not necessarily lead to treatment failure, even with the old cylindrical external-hex implants. With Morse taper implants, these losses are much less frequent, although I have also seen them occur. Sometimes it is easy to identify the cause; other times we simply cannot determine it, so we continue to monitor the patient. As long as there is no peri-implant disease with discharge, the implants remain stable, and the patient is asymptomatic, I would maintain peri-implant gingival control and take serial periapical X-rays and CT scans to monitor bone levels. Frequent clinical examinations (probing and checking for inflammation) are also important, as is verifying occlusal contacts in maximum intercuspation and during lateral excursions. Eliminate premature contacts and, if possible, provide canine protection.
Always assess for bruxism and consider the use of occlusal splints. Check for any uncontrolled systemic conditions such as diabetes or whether the patient is taking sodium alendronate or another bisphosphonate. In your case, I am not sure if the prostheses are splinted, but in my experience, for posterior teeth, a splinted prosthesis has stabilized bone loss on several occasions. I hope this helps, and I apologize if the English is not perfect.
Obviously this is a patient seeking advice here rather than a dentist. I would like to say to this patient, as well as every other dental implant patient, let this image be a wake up call to ask appropriate questions. We have gotten to the point where implant dentistry is no longer a specialty service but rather a significant source of income for a lot of dentists regardless of their level of training or understanding of the materials required for the craft. Because it is a source of “easy money” for a lot of dentists it opens itself up to using a lot of cheap/inexpensive/knock off/copycat/etc… parts and pieces in an effort to improve the bottom line. While all available products might have some form of FDA clearance they are not all the same and this image clearly resembles that of budget friendly hardware. Patient’s have a right to know and they should ask their dentist questions about the products he/she utilizes as definitive hardware and just like having a vehicle restored the final bill should reflect the quality and or authenticity of the hardware being utilized to restore the vessel. Way too many folks in our profession are passing off inexpensive, potentially lower quality, budget friendly hardware to their patients and claiming/charging for premium materials. I knew a guy who served 12 years in federal prison for building structures with cheaper materials than what he claimed on his invoices and I know hundreds of dentists who routinely commit the same crime without any fear of potential consequences. Perhaps in the new year we can all reflect on our practices and usher in an era of honest dentistry where quality matters and our invoices are consistent with the materials being utilized.
I could be wrong but I would suspect that it is a “clone” of Nobel Biocare which is a fancy way justifying a premium price for a discount product. While I am not a fan of Nobel Biocare they are most certainly one of the premium implant manufactures and one that gets frequently copied or cloned. Again I could be wrong but this image looks more like a Nobel clone which may not be a bad thing but it is not valued the same.
Thanks for sharing your thoughts. I’m curious what’s your overall opinion on these dental implants? Do you think they’re a good long-term? I currently have a temporary splint crown and am unsure if I should invest in permanent crowns when the time comes in a few months.
I would rather not get involved but I tend to think most things will work just fine if “we”, meaning folks in the dental profession, will stop looking for things to criticize about other people’s work. Short answer is yes I think you will be fine with what you have but I am likely in the minority on this site…