i have recently grafted with bio-OSS and PuroOSS stabilized with bio guide, closing OAC in the mean time with bio guide. not sure if the dimension of bio guide is big enough. I am a bit scared of using tacks to stabilize the membrane, what do you guys think about this ?
The extraction was completed about 2 months ago, then graft with GBR, then 6 months later CBCT before implant placement for UR7654 region.
i plan to keep the 2mm of connective tissue on the buccal flap , because the bio guide membrane needs to stay on the hard sound bone rather than defect of previous extraction site (with less sound bone), not sure if you guys agree with the flap design, the proximal gingival papillae was preserved as there is some recession on UR7 , which would make suture difficult.
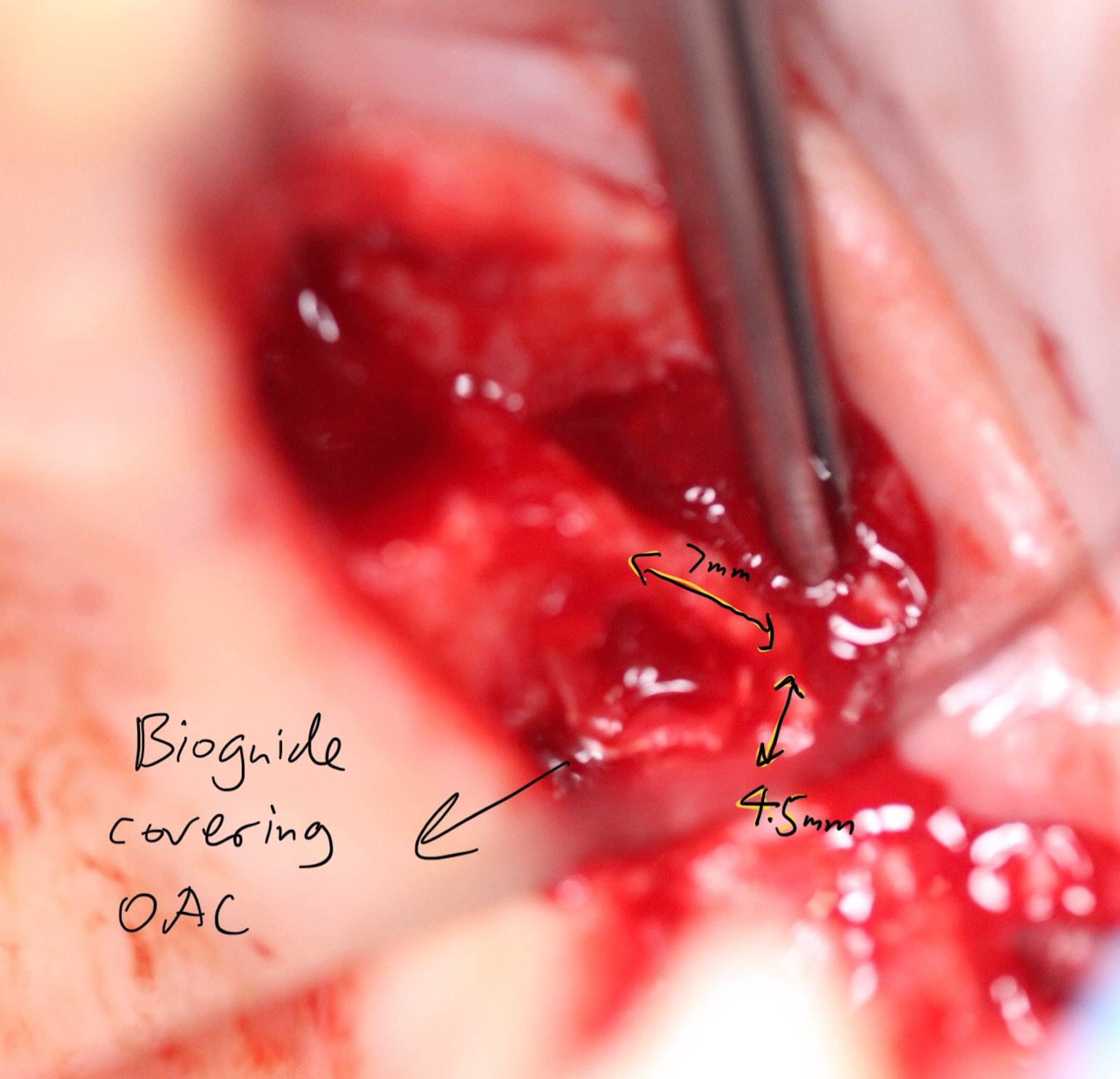
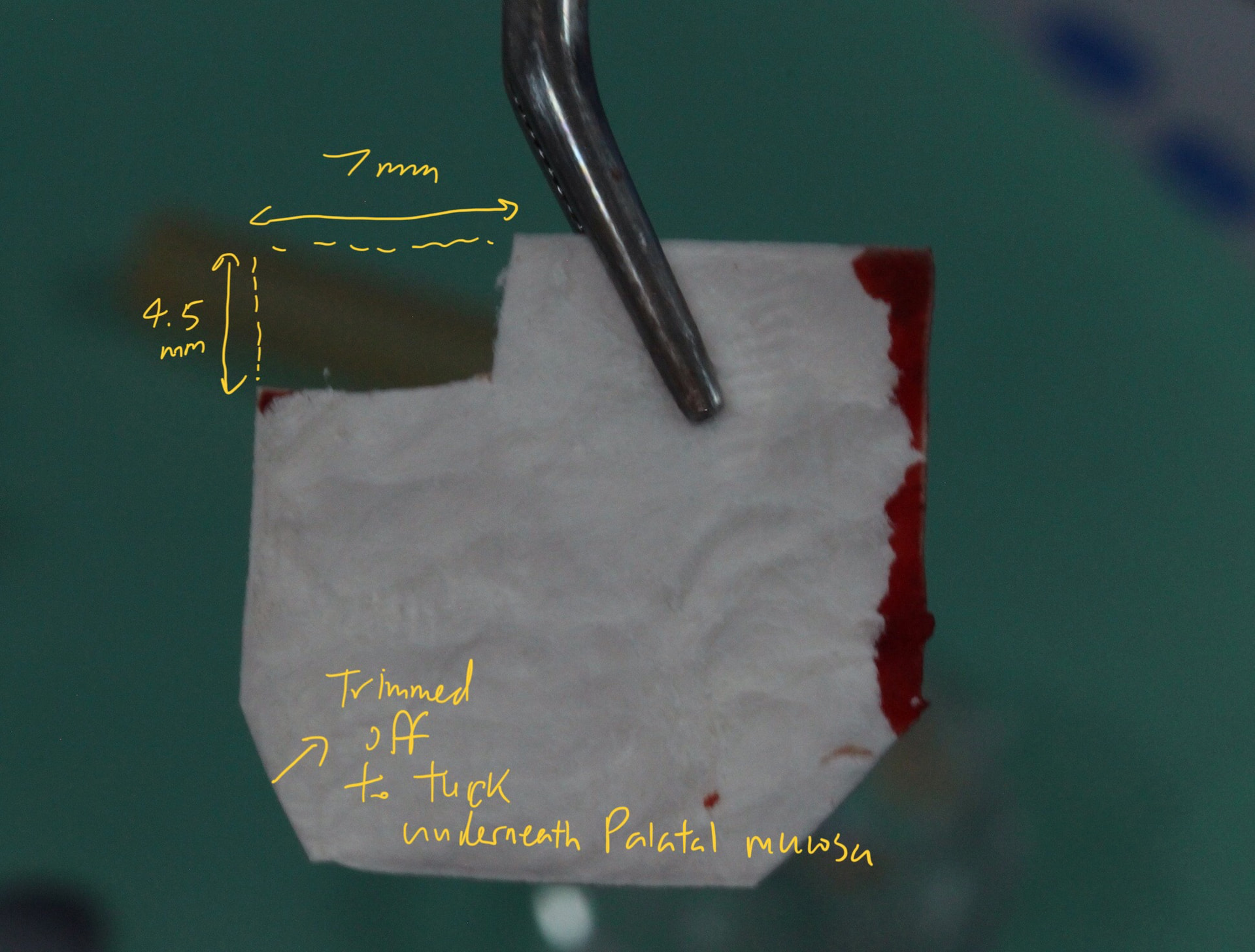
after degranulation bur and curettage of the socket, despite we had done similar things 2 months ago after XLA. there was oral astral communication with per formation of sinus membrane. the defect of the OAC is around 1-2mm, but the crestal defect is 4.5mm by 7mm wide as measured.
( I designed the bio guide dimension, not sure if 4.5mm by 7mm would be able to cover the OAC defect, which is much smaller at the base of the UR6 socket)
Looks like you have done a wonderful job. If I were to suggest anything it would be to go back and review a case that Dr. Gober posted a while back about a palatal roll technique. It might have been beneficial to add additional connective tissue over the ridge and extending to the buccal but this might just be the periodontist coming out in me…
thank you ! the palatal split thickness might be a bit advanced to me so far, this is my first time using bio guide. I did not expect there would be an OAC as pt remains completely asymptomatic so I just thought the bio guide needs to be larger to cover the base defect. would you recommend using Tacks in this case? I am a bit scared of using tacks…
i wouldn’t say the pt has OAF because the gum looks closed after you removed teeth. OAF by definition will have a fistula, meaning a communication between the sinus and the oral cavity. the gum looks healed closed w/o any communication between sinus and oral cavity. but there’s definitely a bony defect on the occlusal of #2 and 4. if i were to use supertacts, i would have used on palatal bone and on buccal bone. i would tap gentle on the buccal b/c the buccal is very thin. but the palatal wall is usually thicker. I think i would have grafted at the time of extraction.
i see, extraction was non surgical as the entire bridge was very mobile but we managed to remove the granuloma extensively. is tacks much better than periostea suture? we used 5-0 vicryl to stabilize the membrane not sure if it is strong enough. some perio specialists recommend 6-0
tack or sutures is surgeon preference, i think. using 5-0 or 6-0 is also surgeon preference. bigger sutures and needles usually easier to nandle/manipulate. but also. b/c the space to pass the suture at the apex of the flap is small. a smaller needle is better. the 6-0 pertain to the suture size not needle size. i usually like thicker suture the better. so less chance to break. for example. i like to use 3-0 chromic and 2-0 PTFE where as most dentist use 4-0.
Personally I only use tacks when doing lateral ridge augmentation and I am overfilling the void. I will use the tacks to stretch and stabilize the membrane but I have never found it necessary if I am only filling a void so I would not have used tacks here. I rarely, if ever, do lateral ridge augmentation (GBR) procedures anymore so I rarely use tacks.
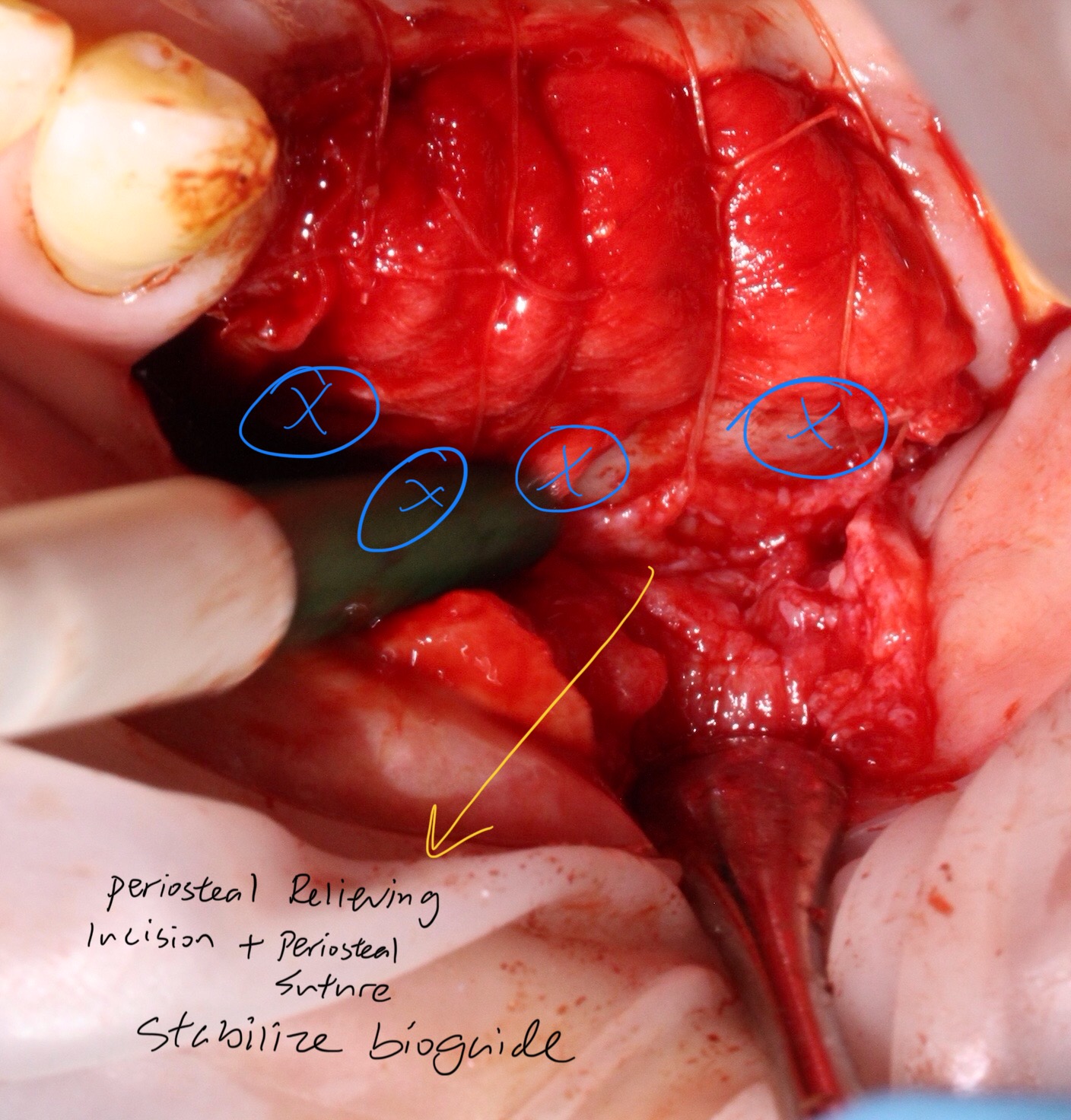
so the technique ‘ periosteal reliving incision and resorbable membrane+ graft + stabilize with periosteal sutures ‘ can also be used for anterior defect GBR cases as well? even other brand of xenograft /allograft or membrane would also work right?
Absolutely!! To be honest with you I rarely stabilize my membranes because most of the time I am just filling a hole with graft material and the membrane is just covering the newly filled hole. My graft is usually stabilized by the anatomy of the defect and the membrane is just a lid… Not true with lateral or vertical GBR though because in these cases the membrane is critical for graft stabilization but for the purpose of filling a hole like you demonstrate here I think you can utilize any variety of techniques and you wont be wrong.
i don’t think all membranes are equal. BioGide is second to none in stretchability and durability. i’ve only found Implant Directs Kontour to match BioGide in these 2 properties. as far as ALLO/XENO. i think all brands are similar and not much different. I actually perform lots of lateral ridge GBR, and i use supertacts all the time. Lots of my patients are asian, and they have very thin bone, atrophy/resorption after prolonged extraction. as a result i have to do lateral GBR all the time.
thank you ! if you do immediate placement in a 4 wall region, i don’t think any membrane is necessary right ? just place graft around the implant in the 4 wall region and cover with temporary cylinder with composite around should be enough , leave for 6 months if using xenograft. 3 months if using allograft / alloplast like ethoss. ?
As a periodontist I was trained to do GTR, which is guided tissue regeneration around teeth. Principals of GTR suggest that a 3 walled defect is extremely predictable and does not require a membrane since there are 3 walls for blood supply and containment/stability. An intact extraction socket is by definition a 4 walled defect and even an extraction requiring the complete obliteration of the buccal plate will leave a 3 walled defect so I don’t believe that membranes are very important for socket preservation… I know most folks routinely use them when grafting a socket but I think that is just because the manufacturer who taught the class suggested more products. Certainly nothing wrong with the routine use of a membrane with intact graft sites but I seriously doubt if it is necessary beyond adding a reimbursable code to the procedure…