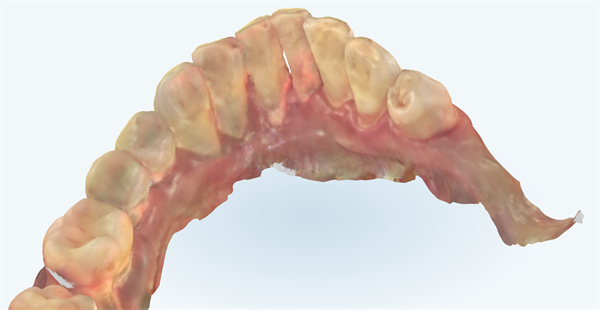
29 and 31, two implants have been placed. The soft tissue on the lingual sides moves up and down due to tongue movement. My question is what is the best way to increase the zone of keratinized tissue on the lingual side? Note: The itero only captured the firm keratinized tissue.
timcarter comments:
Simply reposition the keratinized tissue that lies over the ridge to the buccal or lingual of the healing abutment at the time of placement/uncovering. The exposed portion will fill in and you should be able to easily accomplish your goal
1 Like
timcarter comments:
Another good suggestion is to have the patient brush their teeth at least once a week or so. That iTero managed to capture and highlight plenty of evidence of poor OH...
drtoast15 comments:
Judging the patient helps no one
bromike comments:
the scan was from last year during the initial tx planning stage.
bromike comments:
Did you mean apically repositioned flap on the lingual side? What if both the lingual and buccal require soft tissue grafting?
timcarter comments:
Except that the scan clearly shows signs of plaque induced inflamation. I am not judging the patient but rather suggesting that we don't put the cart before the horse by rushing to place implants in this compromised situation.
dr-g comments:
Why place implant in this perio affected patient ? FGG and/or flap management to help the KT, basic skill in implant dentistry. Tissue is the issue
drtoast15 comments:
This is of no help to the questioner
dr-g comments:
FGG and flap management.
What do you want more from this case with limited info, limited images, no xrays etc.
Do you have a better answer ?
drtoast15 comments:
And you routinely do FGG's on lingual of posterior. lingual areas?
bromike comments:
the scan was from last year during the initial tx planning stage.
dr-g comments:
Routinely, no, but I do it if needed.
Are the implants placed base on ideal prosthetic position ? Was GBR done ?
Could do large FGG on the crest, then expose the implants and split the KT to push some on the lingual and some on the buccal.
If HA already there, submerge the implants under FGG then reopen and split the tissue.
I do soft tissue a lot around implants
dr-g comments:
Share updated situation with clinical pictures, thanks
drtoast15 comments:
Lingually positioned flap
dr-g comments:
So flap management like I said. If you have enough KT to start. If not you add fgg and position the flap to have KT on both side.
I agree with Dr G. Either the lingually positioned KG, after burying it, and at uncovery pushing KG to lingual or a FGG on lingual.